
More Information
Submitted: November 05, 2022 | Approved: November 11, 2022 | Published: November 14, 2022
How to cite this article: Lamia B, Adnen C. How to avoid partial implantation of people with cochlear malformation. Arch Cancer Sci Ther. 2022; 6: 036-037.
DOI: 10.29328/journal.acst.1001031
Copyright License: © 2022 Lamia B, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Keywords: Auditory nerve; Cochlea prosthesis (CI); EAS stimulation; Speech intelligibility

How to avoid partial implantation of people with cochlear malformation
Bouafif Lamia1 and Cherif Adnen2*
1National Institute of Medical Technologies ISTMT, University of Tunis EI Manar, Tunis, Tunisia
2Science Faculty of Tunis, ATSSEE Laboratory, Tunis, Tunisia
*Address for Correspondence: Cherif Adnen, Science Faculty of Tunis, ATSSEE Laboratory, 1060 Tunis, Tunisia, Email: [email protected]
Many advances have been made in recent years in the development of hearing and cochlear implants. These use acoustic and electrical stimulation technologies to improve speech intelligibility for the hearing impaired. However, for cochlear prostheses, the results are not very promising and vary from one patient to another. Certain technical and sometimes physiological problems have limited the expected performances of these devices, especially for children and the elderly. These problems include cochlear malformation and ossification of the auditory channels. This led us to reduce the number of electrodes in order to allow quality deep insertion while preserving the low-frequency acoustic bands of the operated patient.
Advances and limitations of cochlear prosthesis
Psychcoacoustic and deafness measurements in patients implanted with cochlear prostheses have found that successful implantation and performance of implants depend on the choice and placement of the electrodes array in the cochlea. The work of Kumiko [1] showed that the depth of insertion of electrodes, the angle and the intracochlear length of the electrodes as well as their number have an important factor in the success of the surgical operation and the restoration of the patient’s hearing.
Unfortunately, many people with hearing loss have a cochlear malformation or ossification that sometimes prevents the implantation of all electrodes and auditory channels (Figure 1a). In this case, the operation must be completed with a partial extra cochlear implantation in order to not lose the other auditory stimulation channels. Measurements of the rate of insertion of the tympanic ramp on implanted patients showed that for patients with residual hearing at low frequencies, deep insertions with a high number of electrodes led to less good hearing preservation. Yet, when patients without residual hearing were analyzed, a greater insertion depth and a higher number of electrodes gave better performance [2].
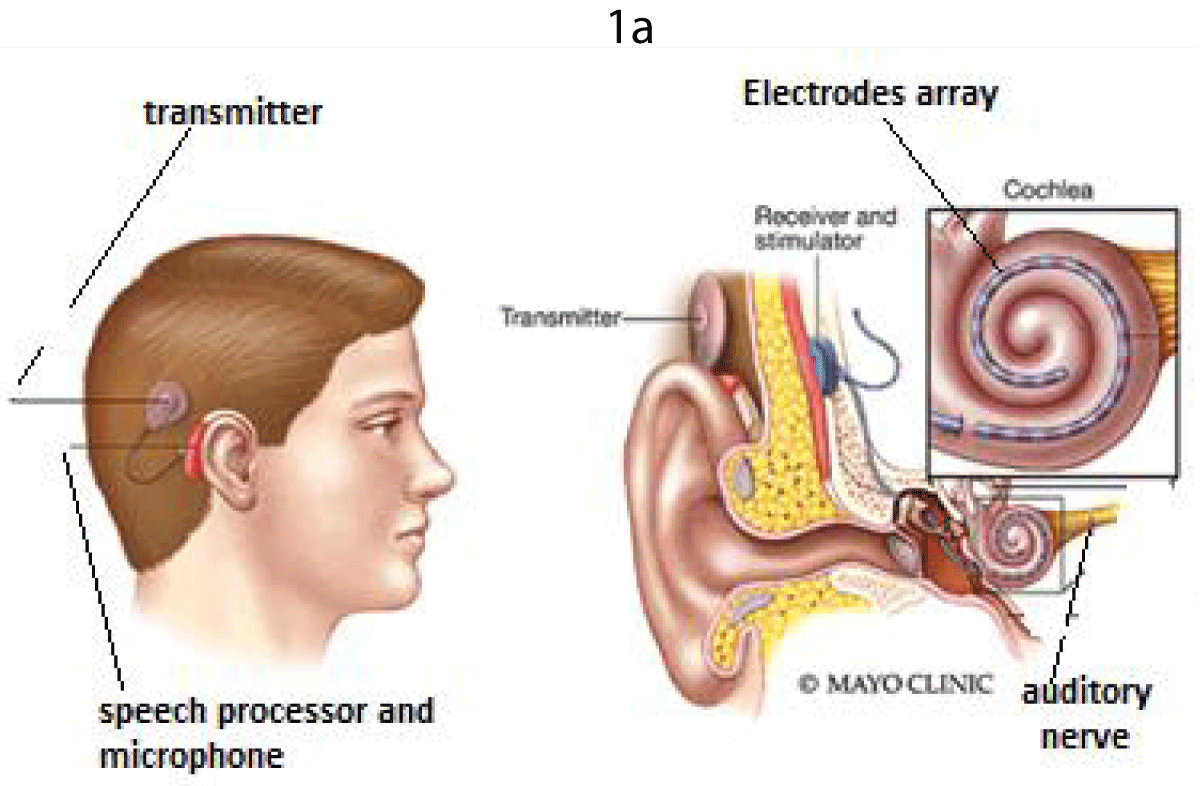
Figure 1a: The cochlear prosthesis and stimuli. (a) Internal structure of a Cochlear implant.
Cochlear implants available today use 16 to 22 electrodes which stimulate only 8 functional sites in the cochlea according to the studies carried out by Dorman in 2002 [3]. Friesen discovered in 2004 that increasing stimulus channels beyond 8 does not provide additional gain in speech understanding. In 2011, Helbig [4] and later Gifford in 2013 [5] showed that adding an acoustic to electric stimulation gives a high advantage, especially under unfavorable listening conditions such as speech in background noise [6].
However, our studies showed that increasing the number of electrodes leads to a complication in the surgical operation and the positioning of the electrode array in the cochlea, electrical interference between neighboring channels as well as higher energy consumption [7]. For this, it is very interesting to encourage the use of electro-acoustic stimulations with a reduced number of electrodes from 4 to 6 (instead of 16) electrically coded on high-frequency electrodes (base) while those of low frequencies (apex) are acoustically stimulated.
Figure 1b represents an example of the electrode stimuli for the speech “Bienvenu” pronounced by a female speaker with 16 kHz of sampling frequency. We can observe the original speech decomposition into 22 channels, their envelopes waveforms then stimuli with a reduction of the number of activated channels (4 to 6 instead of 22). In this case, only four electrodes will be excited (2, 3, 4, 5 and 6) at frequency positions, respectively 212, 281, 362, 507 and 455Hz. Our results have been compared with those from other strategies such as CIS, NoM and SPEAK and proved high efficiency and advantages, especially in the case of residual low frequencies auditory bands [8].
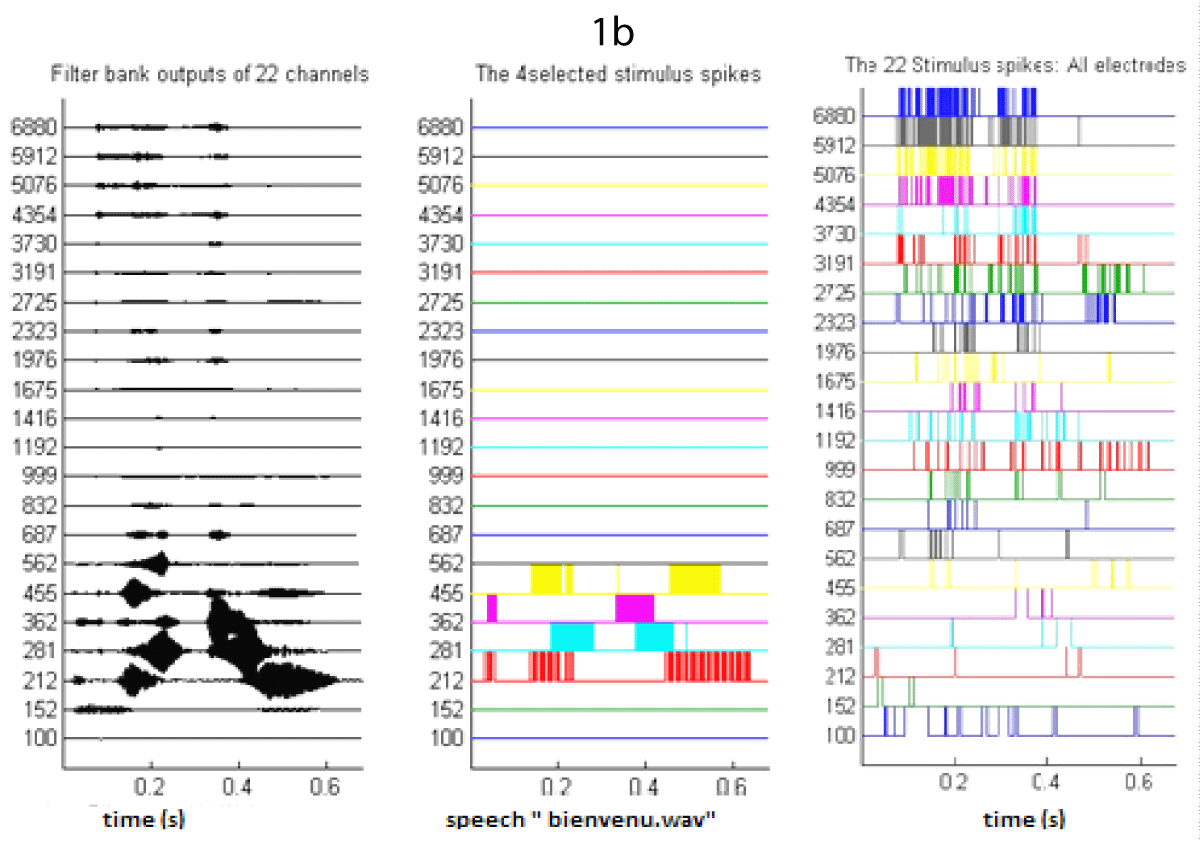
Figure 1b: The cochlear prosthesis and stimuli. b) Electrodes stimuli for the speech “Bienvenu”.
Finally, we can say that the fact of reducing by 50% the number of stimulated channels and electrodes constitutes a big step and an important contribution to the promotion and the implantation of hearing aids. We can say that no credible study has succeeded in stimulating the auditory nerve with only 4 electrodes - 6 electrodes instead of the 12 - 22 currently used. This result is very interesting because it:
- Facilitates surgical implantation
- Decreases the price of the prosthesis
- Decreases the interference between the channels of neighboring electrodes and consequently decreases the noise and enhances the quality of the perceived speech.
- Avoids partial implantation of many people with cochlear malformation or ossification that sometimes prevents the implantation of all electrodes. Actually, in this case, the operation must be completed with a partial extra cochlear implantation in order to not lose the other auditory stimulation channels.
- Yukawa K, Cohen L, Blamey P, Pyman B, Tungvachirakul V, O'Leary S. Effects of insertion depth of cochlear implant electrodes upon speech perception. Audiol Neurootol. 2004 May-Jun;9(3):163-72. doi: 10.1159/000077267. PMID: 15084821.
- O'Connell BP, Hunter JB, Haynes DS, Holder JT, Dedmon MM, Noble JH, Dawant BM, Wanna GB. Insertion depth impacts speech perception and hearing preservation for lateral wall electrodes. Laryngoscope. 2017 Oct;127(10):2352-2357. doi: 10.1002/lary.26467. Epub 2017 Mar 17. PMID: 28304096; PMCID: PMC5825186.
- Dorman MF, Loizou PC. The identification of consonants and vowels by cochlear implant patients using a 6-channel continuous interleaved sampling processor and by normal-hearing subjects using simulations of processors with two to nine channels. Ear Hear. 1998 Apr;19(2):162-6. doi: 10.1097/00003446-199804000-00008. PMID: 9562538.
- von Ilberg C, Kiefer J, Tillein J, Pfenningdorff T, Hartmann R, Stürzebecher E, Klinke R. Electric-acoustic stimulation of the auditory system. New technology for severe hearing loss. ORL J Otorhinolaryngol Relat Spec. 1999 Nov-Dec;61(6):334-40. doi: 10.1159/000027695. PMID: 10545807.
- Gifford RH, Dorman MF, Skarzynski H, Lorens A, Polak M, Driscoll CL, Roland P, Buchman CA. Cochlear implantation with hearing preservation yields significant benefit for speech recognition in complex listening environments. Ear Hear. 2013 Jul-Aug;34(4):413-25. doi: 10.1097/AUD.0b013e31827e8163. PMID: 23446225; PMCID: PMC3742689.
- Vaerenberg B, Péan V, Lesbros G, De Ceulaer G, Schauwers K, Daemers K, Gnansia D, Govaerts PJ. Combined electric and acoustic hearing performance with Zebra® speech processor: speech reception, place, and temporal coding evaluation. Cochlear Implants Int. 2013 Jun;14(3):150-7. doi: 10.1179/1754762812Y.0000000008. PMID: 23321588.
- Bouafif L. Electro-acoustic coding and stimulation strategies. Bookchapter. Noor publishing Editions, Germany. 2016;2-96.
- Croghan NBH, Duran SI, Smith ZM. Re-examining the relationship between number of cochlear implant channels and maximal speech intelligibility. J Acoust Soc Am. 2017 Dec;142(6):EL537. doi: 10.1121/1.5016044. Erratum in: J Acoust Soc Am. 2018 May;143(5):2621. PMID: 29289062.