
More Information
Submitted: July 18, 2023 | Approved: August 02, 2023 | Published: August 04, 2023
How to cite this article: Yousaf M, Ramos R, Gull RI. Quality of Life (QoL) among Pakistani Women with Breast Cancer Undergoing Chemotherapy. Arch Cancer Sci Ther. 2023; 7: 018-026.
DOI: 10.29328/journal.acst.1001037
Copyright License: © 2023 Yousaf M, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.

Quality of Life (QoL) among Pakistani Women with Breast Cancer Undergoing Chemotherapy
Mohammad Yousaf1*, Rita Ramos2 and Rehmatullah Inzar Gull3
1Assistant Director of Nursing, Shaukat Khanum Memorial Cancer Hospital & Research Centre, Lahore, Pakistan
2Master of Arts Nursing program, Department of Faculty Management and Development Studies, UPOU, Philippines
3Nursing Lecturer /Practitioner, Shaukat Khanum Memorial Cancer Hospital & Research Centre, Lahore, Pakistan
*Address for Correspondence: Mohammad Yousaf, Assistant Director of Nursing, Shaukat Khanum Memorial Cancer Hospital & Research Centre, Lahore, Pakistan, Email: [email protected]; [email protected]
Background: Breast Cancer is the most common cancer in women and the quality of life of women with breast cancer is a significant healthcare issue specifically in developing and underdeveloped countries.
Globally quality of Life (QoL) has become an important indicator to measure the outcomes of medical and nursing interventions. The QoL studies have an imperative role in healthcare especially in chronic disease as the latest diagnostic and treatment modalities have increased the survival rates and duration of cancer patients. Similarly, breast cancer itself and its treatment with Chemotherapy, in particular, has many complications and negative impacts on the QoL of cancer women.
Aim: The aim of this study was to assess the QoL of Pakistani women with Breast Cancer patients undergoing chemotherapy and the relationship of QoL with socio-demographic variables.
Methodology: A descriptive cross-sectional correlational study was conducted on 110 female breast cancer patients undergoing chemotherapy. FACIT-B questionnaire was used to assess the quality of life of these patients. Statistical analysis was done by using SPSS version 20 using the Pearson correlation coefficient, Chi-square test, and Spearman’s rho correlation coefficient.
Results: The mean age of participants was (mean ± SD) 42.98 ± 8.98. A significant negative correlation was observed with age and QoL, r = -0.218, p - value 0.022. No significant association was observed between QoL and marital status; education status; and socioeconomic status.
Conclusion: The majority of breast cancer women 59(53.6%) had moderate QoL and Chemotherapy also showed moderate impacts on different domains: physical, functional emotional, social, and sexual well-being of the women.
Breast cancer is the most common cancer in women worldwide and its incidence is increasing, especially in developing countries Musarezai A, Ghasemi TM, Esfahani HN [1]. Generally, this disease is more prevalent in developed countries. However, though Pakistan is a developing country, the Pakistani women have the highest incidence of breast cancer in Asia Khan L [2]. Jemal A, Bray F, Center MM, Ward E, Forman D [3], found out that breast cancer is more common in young females in Pakistan which is contrary to the western countries where it is common in elderly population; approximately one in every nine Pakistani women is likely to suffer from breast cancer, one of the highest incidence rates in Asia.
In the management of patients with breast cancer, chemotherapy or hormonal therapy may also impact self-image, fertility, and libido — all important components of ‘femininity. According to Meneses and Holland [4], “the possible loss of reproductive potential due to toxicities from cancer therapy has a profound impact on quality of life and can increase psychosocial distress among young survivors of breast cancer (p.374)”. The quality of life (QoL) of cancer patients is always disturbed due to this in many ways: physiologically, psychologically, sexually, socially and cognitively. These patients may prefer to isolate themselves and avoid social gatherings and contact by themselves. This can dent social, personal, sexual and psychological image of these patients.
The aim of this study is to examine the quality of life of Pakistani women with breast cancer receiving chemotherapy and to identify factors that affect their quality of life. Secondary objectives are to identify different issues breast cancer women face during chemotherapy course and determine measures to minimize the affliction of these patients to improve the quality of their life.
Significance of the study
This study is very important and innovative in this context as it will explore the Quality of Life of Pakistani breast cancer women undergoing chemotherapy. The study will take advantage of this attempt since there is an unclear exposition of the study’s objective due to lack of local treading and literature. The results of the study may also provide information on this specific issue which may help in the provision of quality nursing care and effective education to breast cancer patients.
This study has taken the role to be equally beneficial for clinical nurses, nurse administrators, nurse educators and nurse researchers. It may explore the educational and counselling needs of such population of patients and be identified and addressed appropriately while receiving the appropriate nursing care. This could also mobilize the nursing force in particular and other healthcare workers to solve patients and family concerns of chemotherapy treatment. Thus, professional understanding by the nurse of the patients may be intensified.
For nurse educators, they may utilize the findings of this study to train their students and provide evidence-based practice in dealing with patients of breast cancer. Proper nursing interventions and programs may be developed by including this to their curriculum in terms of management of oncologic patients. This study may open new roads for nursing research development in terms of discovering new pathways of evidence-based practice in relation to understanding quality of life of oncologic patients.
Research objectives
1. To determine the level of QoL among Pakistani women with breast cancer undergoing chemotherapy.
2. To find out the relationship between QoL of Pakistani women with breast cancer undergoing chemotherapy and their socio-demographic variables.
Research hypotheses
a. There is a relationship between QoL of breast cancer patients undergoing chemotherapy and their socio-demographic variables such as Age, Marital status, Educational status (attainment), and Socioeconomic status.
Null Hypothesis:
b. There is no relationship between QoL of breast cancer patients undergoing chemotherapy and their socio-demographic variables such as Age, Marital status, educational status (attainment), and Socioeconomic status.
Operational definitions of key terms
Quality of Life:
• Quality of life (QoL) was defined as an individual’s perceived physical, mental and social health status affected by Chemotherapy treatment of Pakistani women with breast cancer. This study used the terms ‘health-related quality of life’(HR QoL) and ‘quality of life’ (QoL)interchangeably where applicable.
• According to the WHO [5], QoL is an individual’s perception of their position in life in the context of the culture and value systems in which they live and in relation to their goals, expectations, standards and concerns. It is a broad ranging concept affected in a complex way by the person’s physical health, psychological state, level of independence, social relationships, personal beliefs, and their relationship to salient features of their environment. It was defined operationally from the Functional Assessment of Chronic Illness Therapy (FACIT-B) Measurement System of Pakistani women with breast cancer undergoing chemotherapy.
• Socio demographic profile of Study subjects
a. Age was referred to chronological age in years of the participants of the study.
b. Marital status was referred to married/single/widowed.
c. Educational status was referred to accomplished educational attainment during learning years.
d. Socioeconomic status was referred to gross income per working period (per month income).
Research design
This was a cross- sectional correlational study. This design involves the selection of participants from the target population who have similar condition and/or receive a particular intervention. The descriptive study quantifies the relationship between the factors, as the effect of exposure or an intervention on an outcome. The outcomes were rated in the groups to measure the effects. In this way, groups of human subjects were offered a questionnaire to complete, and assessed for associations between exposures and outcomes. The literature sufficiently supported that the study design was appropriate to explore the quality of life of Pakistani breast cancer women undergoing chemotherapy.
By using this design, the data from the target population (specified population) was collected at single point in time and no follow-up was done. Then, the responses of the participants were discussed to explore the quality of life of Pakistani breast cancer women undergoing chemotherapy and identify the relationships of certain socio-demographic characteristics on quality of life.
Research setting
The Chemotherapy Department (Chemo Bay) of Shaukat Khanum Memorial Cancer Hospital & Research Centre (SKMCH & RC) Lahore-Pakistan was selected as the research setting. Shaukat Khanum Memorial Cancer Hospital & Research Centre (SKMC & RC), a 200-bed tertiary care hospital. Chemotherapy department is a 30 bedded day care unit that provides chemotherapy services to cancer patients including breast cancer patients as a day case.
Selection criteria
The study used purposive sampling method in the determination of its sample count from the target population. The following inclusion and exclusion criterion was used while recruiting participants in this study. All participants were women diagnosed with breast cancer of any disease stage, aged 25 - 65 years old, receiving chemotherapy for at least 1 year (neo-adjuvant). All were able to understand and communicate well, physically, and mentally coherent and newly diagnosed patients who had received at least 6 cycles of chemotherapy. Members of the population with the following characteristics were disregarded to participate in the study: 1) physically or mentally disabled, 2) receiving breast cancer treatment modality other than chemotherapy, 3) recurrent cases, 4) receiving or received chemotherapy at some other hospital/health care agency other than the study setting and 5) presently with existing co-morbidities.
Sample size
Sample size of the study was computed through power analysis for correlations using Cohen’s procedure. G-power software was used to analyze the power with alpha at 0.05, effect size at 0.50 (medium) and power of .80. It required 100 participants to allow achievement of the said power. A 20% oversampling is considered to address possible target sample attritions. Thus, the estimated sample sizes were 121 subjects, but in actual, 110 patients were included due to low attrition rate which was 10% more than the required sample size required to achieved power of 0.80.
Research instruments
Functional Assessment of Cancer Therapy, Breast (FACT-B) version 4.0 questionnaires was used to collect data; permission was taken from the original author of the instrument. The Functional Assessment of Chronic Illness Therapy (FACIT) is a collection of health-related quality of life questionnaires of various chronic diseases. The Functional Assessment of Cancer Therapy-Breast (FACT-B) is a HRQoL instrument under this system, specific to breast cancer patients.
Data collection
A self-administered structured questionnaire, FACT-B (APPENDIX-III) was used as a tool for the data collection. This structured questionnaire was distributed among the selected participants, and they were guided for proper understanding and responding to the question asked. After obtaining responses from the participants, the complete questionnaires were returned to the data collector. The provided responses were not manipulated by the researcher or any other person and for each section it was considered as final.
Ethical considerations
This research was approved by Institutional Review Board of Shaukat Khanum Memorial Cancer Hospital & Research Centre, Lahore.
Statistical treatment
All statistical analyses were performed using the SPSS (Statistical Package for the Social Sciences) software version 20.
1. Descriptive statistics was computed to determine the frequency and percentage of the profile of the respondents. Mean and standard deviations will be computed of QoL.
2. Spearman’s rank- order correlation rho was used to determine the relationship between QoL and the following ordinal variable: educational attainment.
3. Pearson r was used to determine the relationship between QoL and age.
4. Chi- squared test was used to test the difference in proportion in two or more independent groups. This was used in determining the association between QoL and the following nominal variables: marital status, age, educational and socioeconomic status. Fisher exact test was applied where the expected frequency was less than 5. As it is assumed that if frequency in any cell of cross (RXC) tables is less than 5, chi –squared test is not valid.
Descriptive statistics for sociodemographic profile of study participants
In this study, total n = 110 females with breast cancer receiving chemotherapy between the ages 25 and 65 were selected. Socio-demographic profile described in four sub- sections: Age, Marital status, educational attainment, and socioeconomic status. Mean ± SD were calculated for ratio scale data while frequency and percentages were calculated for categorical data.
The socio-demographic profile of females with breast cancer receiving chemotherapy is presented in Table 1. The age of the participants ranged from 25 years to 65 years of age. The mean age was 42.98 ± 8.98. Age was categorized according to the quartiles. Out of 110 female participants, the majority of females 64(58.2%) were from age group of 30 to 50 years while 25(22.7%) females were from age group of >50 years and only 21(19.1%) females were from the age group of < 30 years. In this study it was an observed that majority of women were in age group of 30 - 50 years, that means 64(58.2%) of the participants were in this age range.
| Table 1: Descriptive Statistics for Socio-demographic Profile. | ||
| Socio-demographic Profile | Mean ± S.D | |
| Age (years) | 42.98 ± 8.98 | |
| Socio-demographic Profile | Frequency | Percentage |
| Age Groups | ||
| < 30 Years | 21 | 19.1 |
| 30 - 50 Years | 64 | 58.2 |
| > 50 Years | 25 | 22.7 |
| Marital Status: | ||
| Married | 106 | 96.4 |
| Unmarried | 3 | 2.7 |
| Widow | 1 | 0.9 |
| Educational Status | ||
| Illiterate | 3 | 2.7 |
| Primary | 6 | 5.5 |
| Medal | 15 | 13.6 |
| Matriculation | 39 | 35.5 |
| Intermediate | 17 | 15.5 |
| Graduation | 26 | 23.6 |
| Postgraduate | 4 | 3.6 |
| Socioeconomic Status | ||
| Low <Rs, 10000 | 15 | 13.6 |
| MiddleRs.10000-50000 | 83 | 75.5 |
| High >Rs. 50000 | 12 | 10.9 |
A very high proportion 106(96.4%) of the females were married, only 3(2.7%) were unmarried and 1(0.9%) was widow. Marital status has a great impact on quality of life, partner’s good understanding and sharing affects quality of life very positively. Mean ± SD were calculated for ratio scale data while frequency and percentages were calculated for categorical data.
Majority of the participants were educated. Only 3(2.7%) participants were illiterate. There were 24(21.8%) female who had education below matriculation and 86(78.2%) females had education up to matriculation and above. There were 83(75.5%) females had an income between Rs. 10,000 to 50,000 while 15(13.6%) female had an income more than Rs. 10,000 and only 12 (10.9%) had an income more than Rs. 50,000. The income groups were based on minimum wages defined by Government of Pakistan i.e., Rs.10000 per month (About 100 US dollars).
Quality of Life (QoL) of study participants
Functional Assessment of Cancer Therapy-for Breast cancer (FACT-B) was used as a tool to assess quality of life of women with breast cancer, undergoing chemotherapy from Shaukat Khanum Memorial Cancer Hospital & Research Centre (SKMCH & RC). This scale was used by Li, et al. [6], Pongthavornkamol, et al. [7] and in many other studies and is an approved valid tool. It is a 37-items self-report instrument designed to measure multidimensional quality of Life (QL) in patients with breast cancer with maximum score of 148. Higher scores for the scales and subscales indicate better quality of life. Table 2 describes women’s responses to the FACT-B questionnaire.
| Table 2: Mean Scores and Distribution of Quality of Life Score. | ||
| Quality of Life | Mean ± SD | |
| FACT-B Questionnaire Score | 89.20 ± 18.39 | |
| FACT-B Domains: | ||
| Physical well being | 1.96 ± 1.27 | |
| Social well being | 2.33 ± 1.25 | |
| Emotional well being | 2.66 ± 1.26 | |
| Functional well being | 2.40 ± 1.14 | |
| Breast cancer subscale | 2.36 ± 1.28 | |
| FACT-B Score Level: | Frequency | Percentage |
| < 50% (Poor) | 26 | 23.6 |
| 50 - 70% (Moderate) | 59 | 53.6 |
| > 70% (Good) | 25 | 22.7 |
It consisted of FACT-G (General QOL) 27 items and additional concerns more specific to women with breast cancer 9 items (BCS subscales). General QOL (FACT-B) is divided into five domains: Physical Well-Being: PWB (7 items), Social/Family Well-Being: SWB (7 items), Emotional Well-Being: SWB (6 items), and Functional Well-Being: FWB (7 items) and additional concerns: (10 items).
A. Physical well-being
According to participants’ response mean ± SD 2.23 ± 1.39 were “forced to spend time in bed” 2.6 ± 1.18 were having “lack of energy”, 2.05 ± 1.33 “have pain”, 2.03 ± 1.22 “have nausea”, 1.79 ± 1.23 “bothered by side effects of treatment” and 1.66 + 1.28 have trouble meeting the needs of my family because of my physical condition. The physical well-being domain score was lowest with mean ± SD 1.96 ± 1.27 as compared to all four domains’ scores.
B. Social / family well-being
In social well-being, the participants responses showed that the highest score calculated (mean ± SD) was 3.25 ± 1.01 “accepted illness” 3.08 ± 1.14 “get emotional support from family” 3.07 ± 1.16 were “satisfied with family communication about illness” 2.88 ± 1.39 “feel close to partner (or the person who is main support)” 2.55 ± 1.35 “get support from friends”, 2.27 ± 1.28 “feel close to friends” whereas, 2.23 ± 1.30 were “satisfied with sex life”. Overall the mean ± SD score in the social/family well-being domain was 2.33 ± 1.25.
The social support and belief on God help a lot to improve coping.
The results of the study showed that perceived social support total scores were found to be high (57.41 ± 13.97) and hopelessness scale scores low (5.49 ± 3.80). A reverse, linear relationship between hopelessness scale scores and social support total scores (r = -0.259, p = 0.017) was observed. Hopelessness scores has a statistically significant relationship between education level and having children, occupation, economic status, and spouses’ education level (p < 0.05).
C. Emotional well-being
In emotional well-being category the participants response showed that highest score was given with (mean ± SD) 3.25 ± 1.10 to “losing hope in the fight against illness” 2.88 ± 1.07 were “satisfied with illness coping”, 2.84 ± 1.30 were “worry that condition will get worse”, 2.64 ± 1.44 “worry about dying”, 2.42 ± 1.32 “feel nervous” while, 1.93 ± 1.31 “feel sad” were given lowest score by the study participants. Overall, according to data, the average score of emotional well-being domain was higher 2.66 ± 1.26 compared to all domains.
It was observed that women with chemotherapy reported being more depressed, less satisfied with their life and having higher level of unmet sexuality needs than those without chemotherapy, while this study results showed a relatively high HRQoL score in emotional domain.
Cancer treatments, especially chemotherapy create changes in female body image that may have an effect on emotional relations and psychological status, in addition to alteration in body image. The patients who received chemotherapy had greater mood disturbance (higher negative and lower positive mood scores) than patients who did not receive chemotherapy.
D. Functional well-being
In the functional well-being domain, the participants’ response showed that the highest score with (mean ± SD) 2.92 ± 1.09 was given to “accepted my illness” 2.41 ± 1.13 were “sleeping well” 2.31 ± 1.20 “content with the quality of life right now” 2.29 ± 1.19 “able to enjoy life”, 2.26 ± 1.11 “enjoying the things usually do for fun”, 2.20 ± 1.13 “work (include work at home) is fulfilling” and 1.96 ± 1.16 were “able to work (include work at home)”. Overall the functional well-being domain score was 2.40 ± 1.14 as per participants’ responses.
However, the most common problems in this domain of QoL were not able to having fun (86%), and not able to work (70%) in the patients who were receiving chemotherapy. Significant interactions between chemotherapy and decisional role were observed for the functional well-being subscale and the FACT-G score.
E. Additional concerns
In the additional concerns domain, the highest score with (mean ± SD) 3.11 ± 1.21 was given to “self-conscious about the way dressed”, 3.08 ± 1.02 were “able to feel like a woman”, 3.06 ± 1.09 have “been short of breath”. Similarly, 2.93 ± 1.22 responded that “one or both of arms are swollen or tender” 2.61 ± 1.40 were “bothered by a change in weight”, 1.93 ± 1.23 have “certain parts of the body where experience pain” 1.91 ± 1.28 were “worry about the effect of stress of illness”, 1.84 ± 1.28 “feel sexually attractive. Furthermore, 1.60 ± 1.52 were “bothered by hair loss” and score 1.52 ± 1.53 (mean ± SD) was given to “worry that other members of the family might someday get the same illness”.
Overall, the participants given 2.36 ± 1.28 (mean ± SD) score to this domain in FACT-B questionnaire. According to Hong-li, et al. [7], lower Breast Specific Subscales(BSS) scores were correlated with lower tumour stage, and chemotherapy, but in this study overall highest QOL scores were seen in BSS domain with mean ± SD 2.36 ± 1.28.
The score of FACT-B questionnaire is also categorized as: less 50% score indicates poor quality of life, 50% to 70% indicates moderate quality of life and score >70% indicate good quality of life. There were only 25(22.7%) women who had score >70%, majority of women 59(53.6%) had score between 50 to 70% whereas 26(23.6%) had score < 50%.
High global QOL, defined as equal to the mean score of 60 or greater, was associated with a statistically significant prolongation in survival compared to a score of less than 60 in all patients.
Relationship between quality of life and socio demographic variables
Quality of life and age (Table 3): A correlation test was used to determine the relationship of age and quality of life in breast cancer women. There was statistically significant negative correlation between age and quality of life, r = -0.218, p - value 0.022. As age increases quality of life decreases. A scatter plot summarizes the results in Figure 1. Studies have concluded that there is a negative relationship between age and physical and emotional well-being of breast cancer patients [8-10]. However, some studies had concluded that there was no significant co relation between age and QoL. In another research conducted in Yemen, it was found that age and occupation were not significantly related to QoL. However, a study in China revealed that lower EWB scores were correlated with younger aged women and higher tumour stage (< 40 years) (r = 0.69, p = 0.034; r = 0.84, p = 0.01) (Table 4).
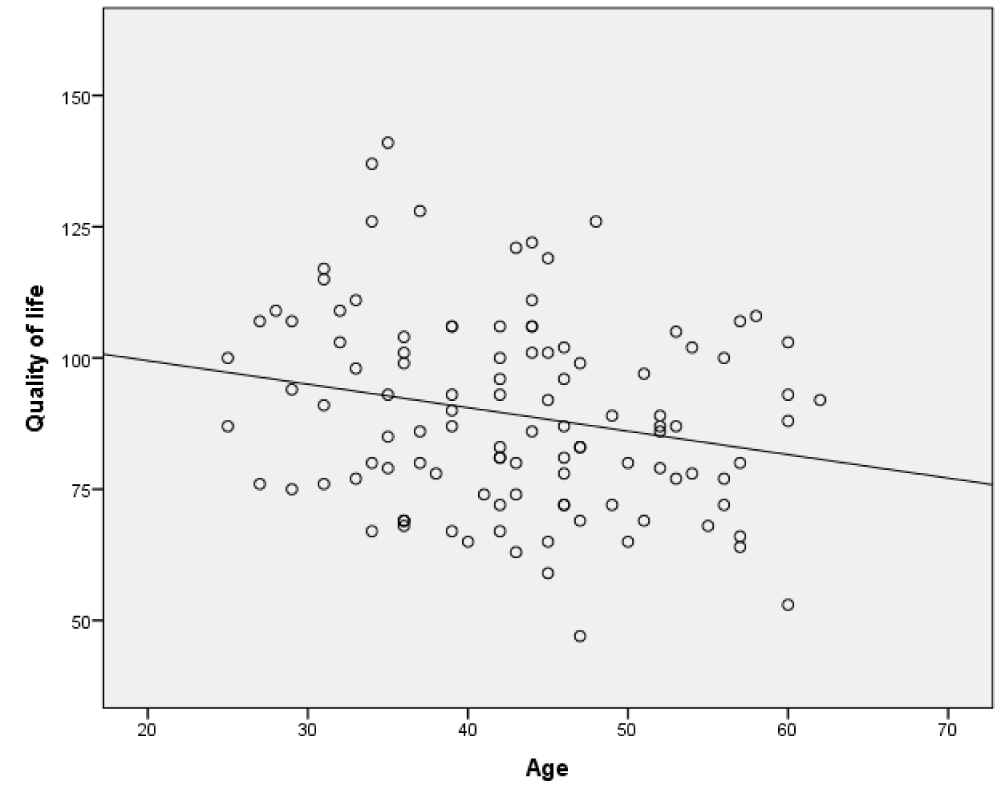
Figure 1: Scatter plot showing the relationship between QoL and age.
| Table 3: Correlation between Age and Quality of life. | |
| Correlation Coefficient (r) | -0.218 |
| p - value | 0.022 |
| Table 4: Distribution of Quality of Life score among different Age Groups. | |||||
| Age Groups | Total n (%) | ||||
| < 30 years n (%) |
30 - 50 Years n (%) |
> 50 Years n (%) | |||
| Quality of Life Score | < 50% | 1 (4.8%) | 19 (29.7%) | 6 (24.0%) | 26 (23.6%) |
| 50 - 70% | 11 (52.4%) | 32 (50.0%) | 16 (64.0%) | 59 (53.6%) | |
| > 70% | 9 (42.9%) | 13 (20.3%) | 3 (12.0%) | 25 (22.7%) | |
| Total | 21 (100%) | 64 (100%) | 25(100%) | 110(100%) | |
| p - value | 0.040 | ||||
Fisher’s exact test: Fisher’s exact test showed that there was significant association between age groups and quality of life scores. Women with age < 30 years had better quality of life score as compared to other age groups. The findings of the present study showed that there was a negative correlation between QoL and age.
Educational status and quality of life (Table 5)
A Coefficient correlation test was used to determine the relationship of education and quality of life in breast cancer women. There was no significant correlation between education and quality of life, r = 0.143, p - value 0.135. A scatter plot summarizes the results in Figure 2. However, no significant relationship was observed between QOL with marital and employment status.
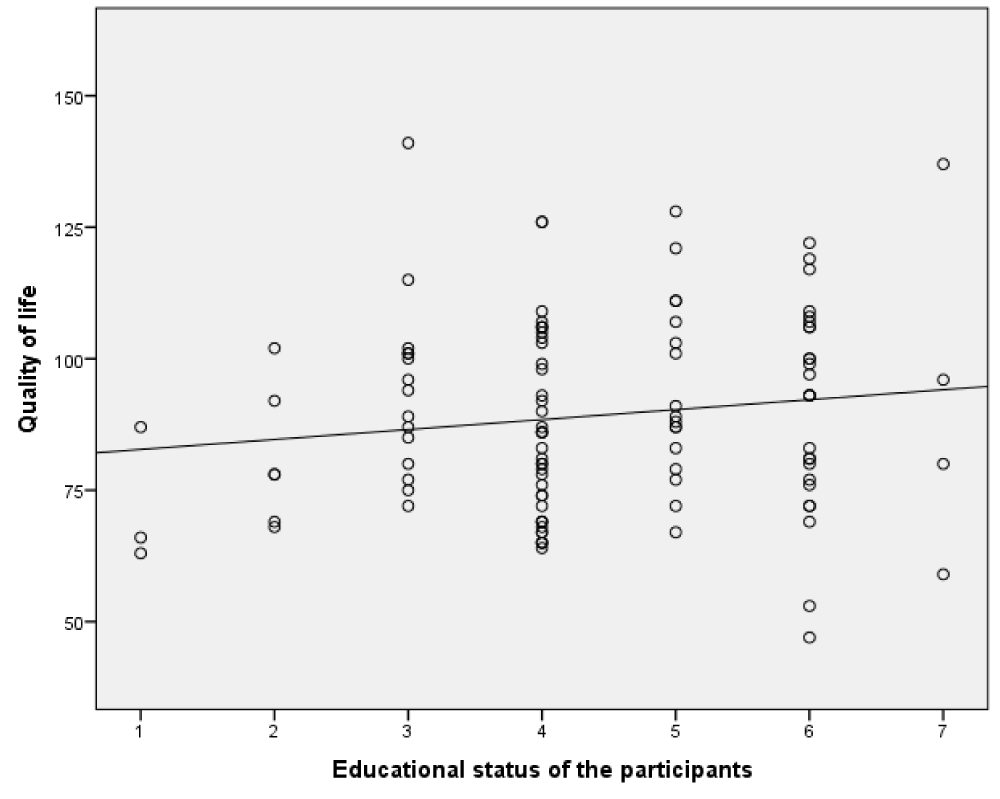
Figure 2: Scatter plot showing the relationship between Education and Quality of Life.
| Table 5: Correlation between Education and Quality of Life. | |
| Correlation Coefficient | 0.143 |
| p - value | 0.135 |
The analysis of variance test, independent t test, Pearson’s and Spearman’s correlation coefficient were used which showed a significant correlation between QoL in Physical Component Summary with gender (p = 0.03), educational level (p = 0.09), and marital status (p = 0.004). Also the Mental Component Summary with educational level (p = 0.01) and economic status (p = 0.02) was significant correlated to QoL. Similarly increased Social Well-Being scores were found significantly correlated with education and occupation (Table 6).
| Table 6: Distribution of Quality-of-Life score according to Educational Status. | ||||
| Educational Status | Total n (%) | |||
| Up to Matriculation n (%) |
Matriculation and above n (%) |
|||
| Quality of Life Score | < 50% | 18 (28.6%) | 8 (17.0) | 26 (23.6%) |
| 50 - 70% | 34 (54.0%) | 25 (53.2%) | 59 (53.6%) | |
| > 70% | 11 (17.5%) | 14 (29.8%) | 25 (22.7%) | |
| Total | 63 (100%) | 47 (100%) | 110(100%) | |
| p - value | 0.190 | |||
Chi-Square test: Generally, the women who had education of matriculation and above they had quality of life score better than those women who education up to matriculation. Pearson Chi-square test showed that there was no significant association between educational status and quality of life scores.
Marital status and quality of life (Table 7)
Fisher’s exact test: Fisher’s exact test showed that there was no significant association between marital status and quality of life scores. There was one woman who was widow and she had quality of life score <50%. There were three women who were unmarried, and they had quality of life score 50 to 70%. Twenty-five women who were married they had quality of life score >70%.
| Table 7: Distribution of Quality of Life score according to Marital Status. | |||||
| Marital Status | Total n (%) | ||||
| Married n (%) |
Unmarried n (%) |
Widow n (%) |
|||
| Quality of Life Score | < 50% | 25 (23.6%) | 0 (0.0%) | 1 (100.0%) | 26 (23.6%) |
| 50 - 70% | 56 (52.8%) | 3 (100.0%) | 0 (0.0%) | 59 (53.6%) | |
| > 70% | 25 (23.7%) | 0 (0.0%) | 0 (0.0%) | 25 (22.7%) | |
| Total | 106 (100%) | 3 (100%) | 1 (100%) | 110(100%) | |
| p - value | 0.247 | ||||
Socioeconomic status and quality of life (Table 8)
Fisher’s exact test: Generally, the women with high socioeconomic status had quality of life score better than middle and low socioeconomic status but Pearson Fisher’s exact test showed that there was no significant association between socioeconomic status and quality of life scores.
| Table 8: Distribution of Quality of Life score according to Socioeconomic Status. | |||||
| Socioeconomic Status | Total n (%) | ||||
| Low n (%) |
Middle n (%) |
High n (%) |
|||
| Quality of Life Score | < 50% | 4 (26.7%) | 18 (21.7%) | 4 (33.3%) | 26 (23.6%) |
| 50 - 70% | 8 (53.3%) | 46 (55.40%) | 5 (41.7%) | 59 (53.6%) | |
| > 70% | 3 (20.0%) | 19 (22.9%) | 3 (25.0%) | 25 (22.7%) | |
| Total | 15 (100%) | 83 (100%) | 12 (100%) | 110(100%) | |
| p - value | 0.866 | ||||
This study shows the relationship between socio-demographic profile of female breast cancer patients’ and quality of life. In women, the most common cancer globally in females is breast cancer and the quality of life of Pakistani women with breast cancer is a significant healthcare issue. This study reveals the relation of socio demographic profile of women with breast cancer receiving chemotherapy with their quality of life. Socio-demographic profile has been described in four sub- sections: Age, Marital status, educational attainment, and socioeconomic status. In this study, majority of females 64(58.2%) were from the age groups of 30 to 50 years old. Only 21(19.1%) females were from the age group of < 30. This study showed that there was negative correlation between age and quality of life (QoL). A Chinese study conducted by Lu, et al. [10], showed the same results. In contrast, Dehkordi A, et al. [11] found that there was no relationship between age and the quality of life. Some research indicates that younger women may suffer poorer QoL following a breast cancer diagnosis that was contrary to this study results. In this study, it was found that there was no significant association between QoL and marital status, education status and socioeconomic status. These results were consistent with the results reported by Dehkordi A, et al. 2009 [12].
A similar study done by Griffiths & Beaver [13], the majority of the participants were younger with a mean age of 41.1. In another study done in Turkey by Gokgoz, et al. [14] on breast cancer patients, the participants were having the mean age 49.37 ± 9.55 years (Mean ± SD) with a range of 27 - 67 years. Safaee, et al. [15], conducted a study in Iran in which 119 patients with breast cancer were interviewed, with a mean age of 48.27 (SD = 11.42), and in another study mean and standard deviation of age was (49.5 ± 9.95) for CT patients [16].
The findings of this study also revealed that majority of women with breast cancer 59(53.6%) had moderate QoL. This result is consistent with Dehkordi A, et al. 2009 [17], study results which showed that the majority of the patients (68%) reported a fairly favorable level of QoL scores.
The score in the physical wellbeing domain of FACT-B questionnaire was the lowest among the all domains of FACT-B Questionnaire. This study also showed that the score in emotional wellbeing was the highest among all the domains of FACT-B questionnaire.
The results of this study are identical with similar previous study reports. A study conducted in South Korea revealed that women experienced significantly poor physical, emotional, social/family, functional well-being and higher breast cancer specific concerns as measured by FACT-B [18]. Eisenbraun, et al. [19] concluded that HRQoL of breast cancer patients is largely affected by chemotherapy and found the loss of appetite, nausea and fatigue. Fatigue was the most common side effect in 65% - 90% of the study subjects.
The quality of life subscales including breast cancer subscale, physical well-being, and emotional well-being, on the other hand, were statistically higher in the group not receiving chemotherapy than in the group receiving chemotherapy [20]. A study conducted in Korea by Hwang, et al. [21] to find out the impacts of Chemotherapy on QoL of breast cancer patients revealed lower scores in Physical well-being and Breast Cancer Scale in participants who received chemotherapy than those who underwent mastectomy and did not receive Chemotherapy. The most common problems in regards to physical problems were anorexia (80%) and fatigue (66%) in patients taking chemotherapy [22].
This study investigated the QOL of breast cancer patients to determine the quality of life among Female Breast Cancer patients based on socio-demographic that includes age, educational attainment, marital status and income [22]. QOL has been used as an endpoint for comparison of treatments in many types of cancer [23]. It is considered an early indicator of disease progression which could help the physicians and nurses in daily), practice to closely monitor the patients [22].
The patients with breast cancer, receiving chemotherapy showed considerable changes in the Global Quality of Life and its various dimensions. HRQoL of breast cancer patients is largely affected by chemotherapy [24] but the women, in this study, considered their state of health and the quality of life satisfactory, which was evidenced by the score of the Global Quality of Life (76.14) [25]. In a study conducted in China showed increased SWB scores were significantly correlated with education and occupation (r = 0.88, p = 0.003; r = 0.76; p = 0.028) [26].
The study results have shown moderate impacts of Chemotherapy in different domains of quality of life: physical, functional emotional, social and sexual well-being. It might be due to a high standard of medical and nursing care, practiced at this oncology center. Almost 60% - 70% patients are treated totally free of any cost, and each and everything is provided from the hospital of the same level as for fully paid patients. This relieves them much of their financial burden of high cost of cancer treatment. No significant correlation was found between QoL and socio demographic variable under study, marital status, income and educational attainment except the negative correlation with the age. Pakistan and most of the Asian countries observe socially joint family system that impacts positively on QoL of cancer patients in all domains. A study conducted in India revealed that 24 (57.1%) patients from nuclear families showed significant levels of depression, in contrast to the 11 (36.2%) patients of joint families (p < 0.05). Thus, family support provided by the members appears to improve the psychological status of a cancer patient [27].
Our overall results were consistent with the results of previous studies, and we found that the patients, who were currently receiving chemotherapy, had lower QoL, physical functioning, role functioning, social functioning, and sexual functioning significantly. Furthermore, symptoms such as fatigue, nausea/vomiting, insomnia, appetite loss, systemic therapy side effects and breast symptoms were seen more frequently among that group.
In a nutshell, it was revealed that most of the participants 59(53.6%) had moderate QoL and Chemotherapy also showed moderate impacts on different domains: physical, functional emotional, social, and sexual well-being of the women. QoL in the physical well-being domain of the participants of this research was the most affected area of these participants while the least affected domain was emotional well-being. In socio-demographic variables, a negative correlation of QoL was found with age whereas there was no significant relationship established with other socio-demographic variables; education, marital status, and income. It might be because of the high standards of care provided in the study setting where free treatment and a strong joint family system support breast cancer woman morally, financially, and physically. There is an intense need for further research studies to compare the effects at a larger scale.
Recommendations
The findings of this study can help medical and nursing staff to plan and improve the quality of breast cancer care in terms of understanding the factors affecting patients’ quality of life. Healthcare professionals must recognize and take the importance of QoL into consideration, besides their treatment, in order to improve the health of breast cancer patients. The results will also help to fill gaps in the current limited knowledge of nursing staff and identify areas in which patients need extra support.
Since there are clear negative effects of cancer and chemotherapy on patients’ QoL, healthcare providers need to focus on designing physio-psychosocial interventions to improve self-care and the QoL and support the cancer patients throughout their illness and chemotherapy. This will improve cancer patients’ adaptation to their disease and emotional well-being. Planned education programs addressing patients’ needs help patients by providing verbal encouragement; introducing patients to positive role models and incorporating pain management guidelines into the delivery of patient care, are important interventions toward improving the quality of life among breast cancer patients.
The study recommends that healthcare professionals should increase their awareness of existential aspects connected with the will to live and assist women and their families in developing coping strategies. Further studies are required to find out the causes of breast cancer in relatively younger females in Pakistan.
- Musarezaie A, Ghasemi TM, Esfahani HN. Investigation the quality of life and its relation with clinical and demographic characteristics in women with breast cancer under chemotherapy. Int J Prev Med. 2012 Dec;3(12):853-9. doi: 10.4103/2008-7802.104856. PMID: 23272284; PMCID: PMC3530303.
- Khan L. Why do we have the highest rates of breast cancer in Asia? 2009. http://www.bluechipmag.com/bc/content_detail.php?content=103
- Jemal A, Bray F, Center MM, Ferlay J, Ward E, Forman D. Global cancer statistics. CA Cancer J Clin. 2011 Mar-Apr;61(2):69-90. doi: 10.3322/caac.20107. Epub 2011 Feb 4. Erratum in: CA Cancer J Clin. 2011 Mar-Apr;61(2):134. PMID: 21296855.
- Meneses K, Holland AC. Current evidence supporting fertility and pregnancy among young survivors of breast cancer. J Obstet Gynecol Neonatal Nurs. 2014 May-Jun;43(3):374-81. doi: 10.1111/1552-6909.12301. Epub 2014 Apr 1. PMID: 24689363.
- WHO. WHOQOL measuring quality of life. Geneva. 1997.
- Li L, Zhu X, Yang Y, He J, Yi J, Wang Y, Zhang J. Cognitive emotion regulation: characteristics and effect on quality of life in women with breast cancer. Health Qual Life Outcomes. 2015 May 6;13:51. doi: 10.1186/s12955-015-0242-4. PMID: 25944458; PMCID: PMC4419411.
- Pongthavornkamol K, Wanavarodom P, Sareeso P, Mahakkakanjana N, Meraviglia M. Improving Health-Promoting Behaviours and Quality of Life through Breast Cancer Support Groups for Thai Women. Pacific Rim Int J Nurs Res 2014; 18(2) 125-137.
- Gokgoz S, Sadikoglu G, Paksoy E, Gunitepe U, Ozcakir A, Bayram N, Bilgel N. Health Related Quality of Life among Breast Cancer Patients: a Study from Turkey. Global Journal of Health Science. 2011; 3:2. www.ccsenet.org/gjhs
- Dehkordi A, Heydarnejad MS, Fatehi D. Quality of Life in Cancer Patients undergoing Chemotherapy. Oman Med J. 2009 Jul;24(3):204-7. doi: 10.5001/omj.2009.40. PMID: 22224186; PMCID: PMC3251183.
- Lu W, Cui Y, Zheng Y, Gu K, Cai H, Li Q, Zheng W, Shu XO. Impact of newly diagnosed breast cancer on quality of life among Chinese women. Breast Cancer Res Treat. 2007 Apr;102(2):201-10. doi: 10.1007/s10549-006-9318-5. Epub 2006 Jul 19. PMID: 16850242.
- Dehkordi A, Heydarnejad MS, Fatehi D. Quality of Life in Cancer Patients undergoing Chemotherapy. Oman Med J. 2009 Jul;24(3):204-7. doi: 10.5001/omj.2009.40. PMID: 22224186; PMCID: PMC3251183.
- Dehkordi A, Heydarnejad MS, Fatehi D. Quality of Life in Cancer Patients undergoing Chemotherapy. Oman Med J. 2009 Jul;24(3):204-7. doi: 10.5001/omj.2009.40. PMID: 22224186; PMCID: PMC3251183.
- Griffiths A, Beaver K. Quality of life during high dose chemotherapy for breast cancer. Int J Palliat Nurs. 1997 May 2;3(3):138-144. doi: 10.12968/ijpn.1997.3.3.138. PMID: 29324094.
- Gokgoz S, Sadikoglu G, Paksoy E, Gunitepe U, Ozcakir A, Bayram N, Bilgel N. Health Related Quality of Life among Breast Cancer Patients: a Study from Turkey. Global Journal of Health Science. 2011; 3:2. www.ccsenet.org/gjhs
- Safaee A, Moghimi-Dehkordi B, Zeighami B, Tabatabaee H, Pourhoseingholi M. Predictors of quality of life in breast cancer patients under chemotherapy. Indian J Cancer. 2008 Jul-Sep;45(3):107-11. doi: 10.4103/0019-509x.44066. PMID: 19018114.
- Alzabaidy FJ,Quality of Life Assessment for Patients with Breast Cancer Receiving Adjuvant Therapy. Cancer Sci Ther. 2012; 4.3. http://dx.doi.org/10.4172/1948-5956.
- Dehkordi A, Heydarnejad MS, Fatehi D. Quality of Life in Cancer Patients undergoing Chemotherapy. Oman Med J. 2009 Jul;24(3):204-7. doi: 10.5001/omj.2009.40. PMID: 22224186; PMCID: PMC3251183.
- Hwang SY, Chang SJ, Park BW. Does chemotherapy really affect the quality of life of women with breast cancer? J Breast Cancer. 2013 Jun;16(2):229-35. doi: 10.4048/jbc.2013.16.2.229. Epub 2013 Jun 28. PMID: 23843858; PMCID: PMC3706871.
- Eisenbraun J, Scheer R, Kröz M, Schad F, Huber R. Quality of life in breast cancer patients during chemotherapy and concurrent therapy with a mistletoe extract. Phytomedicine. 2011 Jan 15;18(2-3):151-7. doi: 10.1016/j.phymed.2010.06.013. Epub 2010 Aug 19. PMID: 20724129.
- Pongthavornkamol K, Wanavarodom P, Sareeso P, Mahakkakanjana N, Meraviglia M. Improving Health-Promoting Behaviors and Quality of Life through Breast Cancer Support Groups for Thai Women. Pacific Rim Int J Nurs Res. 2014; 18(2):125-137.
- Hwang SY, Chang SJ, Park BW. Does chemotherapy really affect the quality of life of women with breast cancer? J Breast Cancer. 2013 Jun;16(2):229-35. doi: 10.4048/jbc.2013.16.2.229. Epub 2013 Jun 28. PMID: 23843858; PMCID: PMC3706871.
- Alzabaidy FJ. Quality of Life Assessment for Patients with Breast Cancer Receiving Adjuvant Therapy. Cancer Sci Ther. 2012:4.3. http://dx.doi.org/10.4172/1948-5956.
- Ochayon L, Zelker R, Kaduri L, Kadmon I. Relationship between severity of symptoms and quality of life in patients with breast cancer receiving adjuvant hormonal therapy. Oncol Nurs Forum. 2010 Sep;37(5):E349-58. doi: 10.1188/10.ONF.E349-E358. PMID: 20797943.
- Eisenbraun J, Scheer R, Kröz M, Schad F, Huber R. Quality of life in breast cancer patients during chemotherapy and concurrent therapy with a mistletoe extract. Phytomedicine. 2011 Jan 15;18(2-3):151-7. doi: 10.1016/j.phymed.2010.06.013. Epub 2010 Aug 19. PMID: 20724129.
- Lobo SA, Fernades AF, Almeida PC, Carvalho ML, Sowada NO. Quality of life in women with breast cancer undergoing chemotherapy. Acta paul. enferm. São Paulo. 2014; 27:6; 151–157. http://www.scielo.br/scielo.php?pid=S0103-21002014000600554&script=sci_arttext&tlng=en Pages
- Hong-Li C, Xiao-Chun W, Jiang-Bin W, Jing-Bo Z, Yao W. Quality of life in patients with breast cancer and their rehabilitation needs. Pak J Med Sci. 2014 Jan;30(1):126-30. doi: 10.12669/pjms.301.3952. PMID: 24639845; PMCID: PMC3955556.
- Chintamani, Gogne A, Khandelwal R, Tandon M, Jain S, Kumar Y, Narayan N, Bamal R, Srinivas S, Saxena S. The correlation of anxiety and depression levels with response to neoadjuvant chemotherapy in patients with breast cancer. JRSM Short Rep. 2011 Mar 14;2(3):15. doi: 10.1258/shorts.2010.010072. PMID: 21541083; PMCID: PMC3086323.