
More Information
Submitted: May 29, 2026 | Accepted: June 05, 2026 | Published: June 08, 2026
Citation: Ma Y, Lu Z , Sun Y, Li J. Application of In vitro Reconstructed 3D Biomimetic Tumor Microenvironment Models in Cancer Research. Arch Cancer Sci Ther. 2026; 10(1): 16-27. Available from:
https://dx.doi.org/10.29328/journal.acst.1001051
DOI: 10.29328/journal.acst.1001051
Copyright license: © 2026 Ma Y, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Keywords: Tumor microenvironment; 3D biomimetic tumor models; Tumor spheroids; Tumor organoids; Tumor-on-a-chip; Precision oncology

Application of In vitro Reconstructed 3D Biomimetic Tumor Microenvironment Models in Cancer Research
Yinuo Ma1,2, Zhiyuan Lu1*, Yili Sun1-3* and Jia Li1-3*
1School of Pharmacy, Shandong First Medical University, Jinan 250000, Shandong, China
2Shandong Laboratory of Yantai Drug Discovery, Bohai Rim Advanced Research Institute for Drug Discovery, Yantai 264117, Shandong, China
3State Key Laboratory of Drug Research, Shanghai Institute of Materia Medica, Chinese Academy of Sciences, Shanghai 201203, China
*Address for Correspondence: Zhiyuan Lu, School of Pharmacy, Shandong First Medical University, Jinan 250000, Shandong, China, Email: [email protected]
Yili Sun, Shandong Laboratory of Yantai Drug Discovery, Bohai Rim Advanced Research Institute for Drug Discovery, Yantai 264117, China, Email: [email protected]
Jia Li, State Key Laboratory of Drug Research, Shanghai Institute of Materia Medica, Chinese Academy of Sciences, Shanghai 201203, China, Email: [email protected]
Cancer is a highly heterogeneous and dynamic disease whose progression, metastasis, therapeutic resistance, and immune escape are strongly regulated by the tumor microenvironment (TME). However, conventional two-dimensional (2D) cell culture systems and animal models often fail to recapitulate the structural organization, multicellular interactions, biochemical gradients, and mechanical properties of native tumors, thereby limiting the translational efficiency of preclinical cancer research and drug development. In recent years, in vitro three-dimensional (3D) biomimetic tumor models-including tumor spheroids, tumor organoids, and tumor-on-a-chip systems—have emerged as powerful platforms for reconstructing physiologically relevant tumor microenvironments and investigating complex tumor behaviors.
In this review, we systematically summarize the construction principles, biological characteristics, advantages, and limitations of major 3D biomimetic tumor models. We further discuss their recent applications in drug screening, precision medicine, tumor heterogeneity research, cancer stem cell investigation, metastasis, therapeutic resistance, and immunotherapy evaluation. Particular emphasis is placed on the comparative advantages of different 3D systems in modeling dynamic tumor–microenvironment interactions and supporting translational oncology research. Additionally, we will discuss the current problems of vascularisation, extracellular matrix biomimetics, experimental reproducibility, standardisation, and large-scale clinical translation. Finally, we present some new directions for future work, including three-dimensional bioprinting, multi-omics technology, artificial intelligence, and multi-organ-on-a-chip platforms, which may further improve the physiological relevance and predictive power of next-generation tumor models.
In short, this review has listed the current progress of 3D biomimetic tumour modelling and discussed some prospects for its use in mechanistic studies of cancer, drug discovery, etc.
Cancer is still one of the top causes of death and illness in the world today, and many countries have not been able to solve this problem [1]. Although there has been some progress in molecular oncology, targeted therapy, and immunotherapy recently, the overall clinical success rates for anti-cancer drugs at present are still relatively low. One reason for the above deficiency is that there are currently no preclinical tumour models that can accurately reproduce the complexity and heterogeneity of the human TME. Conventional 2D monolayer cultures and animal models have served as the standard experimental platforms for cancer research for a long time; however, both systems are significantly lacking in reproducing the structural, biochemical, and mechanical features of human tumours in vivo [2-4].
Traditional 2D cell culture systems are simple, cost-effective, and suitable for high-throughput screening, but they cannot replicate the three-dimensional spatial arrangement, extracellular matrix (ECM) interactions, oxygen and nutrient gradients, and multicellular communication of tumors in vivo [5]. Cancer cells in 2D culture often show changes in shape and polarity, metabolism, gene expression, and drug resistance compared with those in patient tumours. Therefore, many therapeutic agents with good efficacy in 2D systems fail to translate effectively into clinical practice. Animal models, such as genetically modified mouse models and patient-derived xenografts (PDXs), are more physiologically relevant than 2D cultures and can retain some characteristics of systemic tumour growth. Inter-species differences in immune regulation, stromal composition and metabolism, and pharmacokinetics have also reduced the predictability of human therapeutic response. Animal models are also costly, time-consuming, ethically difficult, and not easy to standardize for large-scale drug screening applications[6].
Based on the above data, the progression of tumors is not only due to genetic mutations in the cancer cells but is also influenced by other factors in the TME. TME is a very dynamic and heterogeneous ecosystem that includes cancer cells, cancer-associated fibroblasts (CAFs), endothelial cells, immune cells, mesenchymal stromal cells, components of the extracellular matrix, soluble cytokines, and biophysical cues[7,8]. The links between the above components are necessary for tumour initiation, angiogenesis, immune evasion, metastasis, and drug resistance[7,9,10]. There is also heterogeneity in tumours at multiple levels, such as intertumoural heterogeneity among different patients and intratumoural heterogeneity within the same tumour. The intricate cellular and molecular interactions are difficult to observe accurately with the current experimental model, so more biomimetic in vitro systems are needed urgently [6].
Recently, in vitro-reconstructed 3D biomimetic tumour models have appeared in cancer research and personalised medicine. Compared with the traditional model, a 3D system can better reflect the structural organisation of tumours in nature, as well as cell-cell and cell-matrix interactions and biochemical gradients, etc. Among these technologies, tumor spheroids, tumor organoids, and tumor-on-a-chip systems are three representative types of 3D biomimetic models with progressively higher degrees of structural and functional complexity. Tumor spheroids can form hypoxic gradients and multicellular interactions that resemble avascular tumor regions. Tumour organoids keep the histopathological and genomic traits of patient tumours and are being used to develop personalised medicine and drug-sensitivity prediction tools. Tumor-on-a-chip systems are now also equipped with microfluidic perfusion and vascular interfaces to replicate the dynamic state and multicellular communication in the TME.
Importantly, the new three-dimensional models of life are not just continuous extensions of the old culture system; they have also altered our understanding of cancer at the cellular level. Through the reconstruction of key features of the TME, 3D biomimetic models have enabled mechanistic studies of cancer stem cell plasticity, epithelial-mesenchymal transition (EMT), metabolic reprogramming, immune evasion, and therapy resistance. In addition, the combination of patient-derived models with single-cell sequencing, spatial omics, artificial intelligence (AI) and 3D bioprinting technology is also progressing in the development of next-generation tumor platforms with stronger clinical predictive power.
Although many studies have summarised individual 3D culture technologies, most are still descriptive and do not focus on their complementary roles. The three main problems in the current research are as follows: (1) There is a lack of a systematic comparison study of different 3D platforms for reconstructing the TME; (2) Insufficient integration of model characteristics with specific scientific questions and clinical translation needs; and (3) Fragmented analysis of new interdisciplinary technologies and their synergistic effect.
To fill the above deficiencies, this review offers the following three particular contributions: First, we have organized a comprehensive comparison of tumour spheroids, organoids and tumour-on-a-chip systems based on their capacity to reconstruct essential TME components (such as hypoxia gradients, extracellular matrix, immune interactions), rather than focusing only on technical characteristics. Second, we build a “model characteristic-scientific problem-clinical application” matching framework to guide the selection of a suitable model. Thirdly, we will analyze the three main systemic bottlenecks in the clinical translation of this technology (physiological accuracy, standardisation, accessibility) and propose practical countermeasures by combining biomaterials, vascular engineering, and artificial intelligence. This paper hopes to offer a critical and forward-looking direction for the development of next-generation tumour models.
In vitro reconstructed 3D biomimetic tumor microenvironment models
In recent years, three representative in vitro 3D biomimetic tumor models, including tumor spheroids, tumor organoids, and tumor-on-a-chip systems, have been widely developed and applied in cancer research (Table 1). These models exhibit progressively increasing levels of structural complexity and biomimetic fidelity, ranging from simple multicellular aggregates to highly integrated microphysiological platforms. Compared with conventional 2D culture systems, 3D biomimetic models more effectively reconstruct key features of the TME, including cell–cell and cell–matrix interactions, oxygen and nutrient gradients, biomechanical signaling, and multicellular heterogeneity [11].
| Table 1: Comparison of 3D tumor models. | ||||||||
| Model | Cell Source | Typical Size | ECM Dependency | Physiological Fidelity | Throughput | Cost | Strengths | Limitations |
| Tumor Spheroids | Cancer cell lines | 100-500 μm | Low | Medium | High | Low | Easy fabrication, high reproducibility, suitable for high‑throughput screening | Poor heterogeneity, limited TME complexity |
| Tumor Organoids | Patient tumor tissues/stem cells | 100-500 μm | High(Matrigel/ECM) | High | Medium | Medium | Preserve genomic/phenotypic heterogeneity, predict clinical drug response | Long culture period, unstable passaging, matrix variation |
| Tumor-on-a-Chip | Cell lines/ patient-derived cells | Customizable | High(hydrogel/perfusion) | Highest | Medium-High | High | Recapitulate perfusion, shear stress, vascular invasion, multi‑cellular crosstalk | Complex fabrication, low standardization, scaling challenges |
Among the above systems, tumor spheroids are relatively simple and low-cost platforms for high-throughput drug screening and cancer stem cell studies. Tumor organoids better preserve patient-specific histological and genetic characteristics, thereby supporting disease modeling and precision oncology applications. Tumor-on-a-chip platforms further integrate microfluidic perfusion, vascular interfaces, and dynamic mechanical stimulation, enabling more physiologically relevant simulation of tumor progression and therapeutic response. Although each model possesses distinct advantages and limitations, together they compensate for many deficiencies of conventional 2D culture and animal models and provide increasingly powerful tools for mechanistic cancer research and translational oncology.
Tumor spheroids
Tumor-derived spheroids, also termed multicellular tumor spheroids (MCTS), are the earliest and most widely used 3D tumor model. Sutherland and others were the first to show in 1971 that spheroids spontaneously form hypoxic gradients and necrotic cores identical to those in avascular solid tumors [12]; thus, this system has been used as the gold standard for initial drug screening and research on tumor metabolism. When the diameter of MCTS exceeds about 100 µm, oxygen and nutrient diffusion become spatially limited, and a microenvironmental gradient similar to that in solid tumors develops. A typical necrotic centre has formed in the spheroid; the centre is quiescent, and the periphery is characterised by active division of malignant cells. Different places have supplied various materials for the study of hypoxia-induced cancer proliferation, angiogenesis, metabolic alteration, and drug resistance.
MCTS can be generated as either homotypic spheroids consisting solely of tumor cells or heterotypic spheroids by co-culturing with stromal cells such as fibroblasts, endothelial cells, or immune cells. Compared with traditional 2D monolayer cultures, tumor spheroids can reproduce the multicellular structure, cell-cell interactions, ECM deposition, and metabolic gradients in the TME of a tumor better [13,14]. In addition, the dense cellular organization and ECM accumulation within spheroids contribute to multicellular drug resistance (MCDR) by limiting the penetration of chemotherapeutic agents and immune cells [15].
Another important application of MCTS is the enrichment and investigation of cancer stem cells (CSCs). Studies have demonstrated that tumorsphere culture under non-adherent conditions significantly increases the proportion of cells exhibiting stem-like phenotypes, including CD44+/CD24− populations [16]. Therefore, tumor spheroids are widely used to evaluate CSC-associated characteristics such as self-renewal capacity, differentiation potential, tumor initiation, and therapeutic resistance, thereby providing valuable tools for studying tumor heterogeneity and recurrence mechanisms.
Due to their low cost, ease of maintenance, and compatibility with high-throughput analysis, tumor spheroids have been extensively applied in drug screening and mechanistic cancer research [17]. Compared with more complex 3D systems such as tumor organoids and tumor-on-a-chip platforms, MCTS are relatively simple to establish and suitable for large-scale experimental studies (Figure 1).
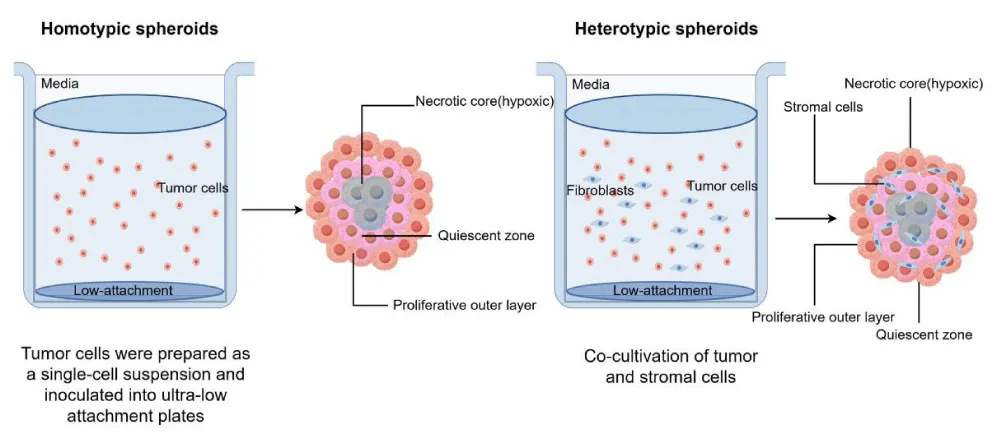
Figure 1: Schematic illustration of tumor spheroid formation and multicellular organization. Homotypic spheroids are generated from tumor cells alone, whereas heterotypic spheroids incorporate stromal components to partially reconstruct tumor microenvironmental interactions.
Tumor organoids
Although tumor spheroids have been widely used for decades, their inability to preserve patient-specific tumor heterogeneity limits their clinical translational value. The breakthrough came in 2009 when Sato, et al. first established long-term cultured intestinal organoids from adult stem cells [18], followed by the first generation of patient-derived tumor organoids (PDOs) in 2011 [19]. These landmark studies laid the foundation for modern organoid technology and revolutionized personalized cancer research. Organoids are three-dimensional tissue constructs derived from stem cells, organ-specific progenitor cells, or dissociated patient tumor tissues and are cultured within ECM-based systems under defined conditions (Figure 2). Compared with conventional spheroid models, tumor organoids exhibit higher physiological relevance and better preserve the histopathological architecture, genomic landscape, mutation profiles, and therapeutic responses of primary tumors [20,21].
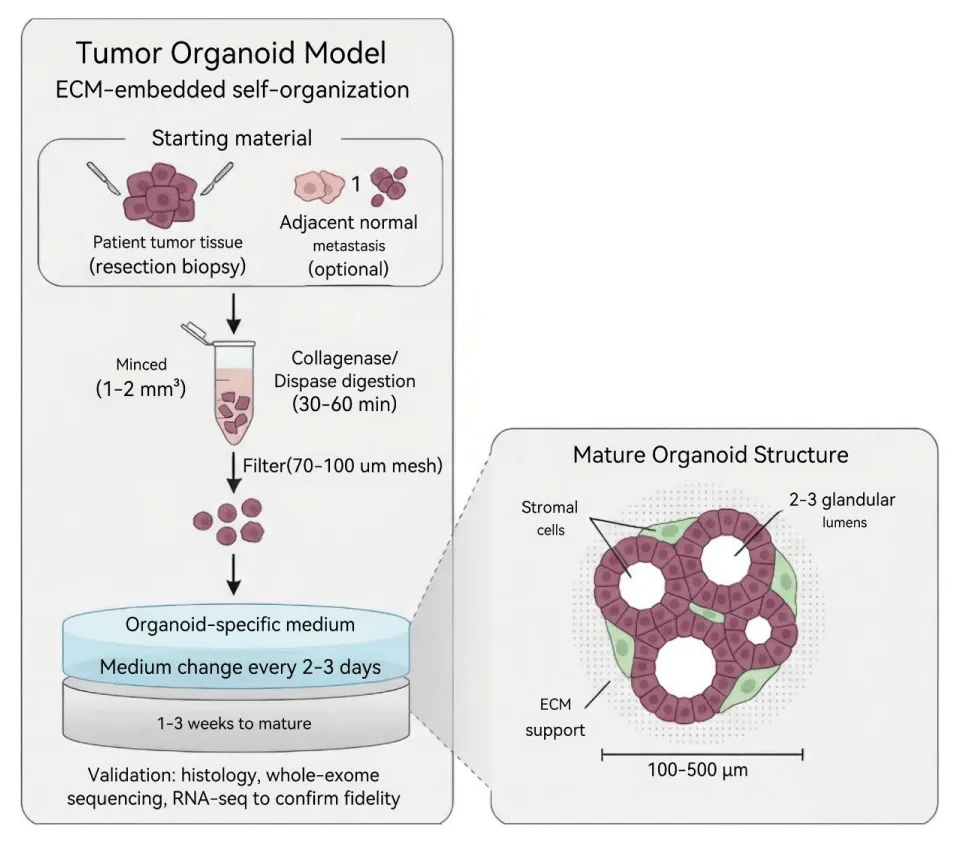
Figure 2: Schematic illustration of the establishment and structural organization of tumor organoids. Patient-derived tumor tissues are dissociated and cultured in ECM-based systems to generate self-organized organoids. Mature organoids partially reconstruct glandular architecture, stromal interactions, and multicellular heterogeneity observed in native tumors.
To date, tumor organoids have been successfully established from a wide spectrum of human malignancies, including lung, breast, colorectal, ovarian, prostate, and gastric cancers [22-27]. Compared with PDX models, organoids require smaller tissue samples, shorter establishment time, and lower experimental costs while maintaining important tumor characteristics during in vitro expansion [22,28]. In particular, PDOs provide valuable platforms for investigating tumor heterogeneity, therapeutic sensitivity, and mechanisms of drug resistance, thereby showing considerable promise in translational cancer research and personalized medicine [29,30].
In addition to preserving patient-specific tumor features, organoid systems also facilitate mechanistic studies of tumor progression, cancer stem cell plasticity, and tumor–microenvironment interactions. Additionally, organoid biobanks from various patients have enabled large-scale studies of intertumoral heterogeneity and supported personalised therapeutic assessments [31].
Tumor-on-a-chip
Organ-on-a-chip (OOC) platforms are microfluidic culture systems that have been used to build organ-specific physiological functions in vitro by adding living cells, extracellular matrix materials, and dynamic mechanical stimuli. With the development of the classic lung-on-a-chip model [32], Many OOC systems have been built to study diseases and drugs on a microscale, including liver-on-a-chip, heart-on-a-chip, kidney-on-a-chip, and intestine-on-a-chip models [33-39].
Based on the above progress, tumour-on-a-chip (TOC) systems have gradually developed and are now being used to study the dynamic tumour microenvironment and test anti-cancer drugs [40-42]. Compared with traditional static 3D cultures, TOC platforms are now capable of microfluidic perfusion, vascular interfaces, biomechanical stimulation, and multicellular co-culture to present more physiologically relevant models of tumour growth and drug response. By incorporating tumor cells together with stromal cells, endothelial cells, or immune cells within ECM-based microchannels, TOC systems can partially reproduce tumor angiogenesis, immune cell infiltration, metastatic dissemination, and drug transport processes observed in vivo [43-45].
Importantly, tumor-on-a-chip platforms provide unique advantages for investigating dynamic tumor–microenvironment interactions. Continuous fluid perfusion and controlled shear stress allow these systems to mimic vascular circulation and biochemical gradients that are difficult to reconstruct in conventional spheroid or organoid cultures. In addition, multiple chip devices can be operated in parallel for multiplexed drug screening and personalized therapeutic evaluation using patient-derived tumor cells. These features have promoted the application of TOC platforms in precision oncology and the development of novel drug delivery systems (NDDS) [46-48] (Figure 3).
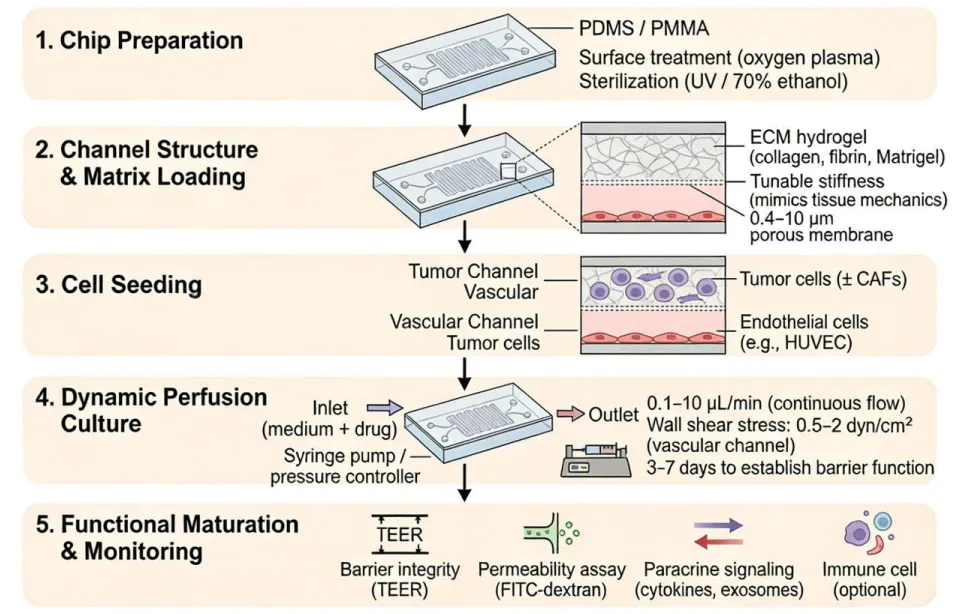
Figure 3: Schematic illustration of the construction and application of tumor-on-a-chip systems. Microfluidic chips are fabricated using biocompatible materials and integrated with extracellular matrix hydrogels, tumor cells, stromal cells, and vascular components to reconstruct dynamic tumor microenvironments under continuous perfusion conditions.
Comparative advantages and limitations of different 3D models
Although tumor spheroids, tumor organoids, and tumor-on-a-chip systems all belong to the category of 3D biomimetic tumor models, they differ substantially in structural complexity, biomimetic fidelity, experimental scalability, and translational applicability [11]. These models should therefore not be regarded as mutually substitutive systems, but rather as complementary platforms suitable for different stages of cancer research and drug development. Compare the strengths and weaknesses of the two, select an appropriate experimental model, and identify existing issues in translational oncology at this time.
Tumour spheroids are relatively simple and readily available 3D tumour models. They can be rapidly generated by the conventional cancer cell line system under low-adhesion or suspension culture conditions, have good reproducibility, are low-cost, and are suitable for high-throughput drug screening. Spheroids also have some attributes of solid tumors, such as hypoxia gradients, limited nutrient diffusion, necrotic cores, and multicellular drug resistance. The above features are suitable for research on tumor metabolism, enrichment of CSCs and therapeutic resistance, and nanoparticle penetration. In addition, heterotypic spheroids formed by co-culture with stromal cells can partially reproduce cell-cell interactions in the TME [49].
Tumor spheroids are also relatively limited in some respects. Most spheroids are derived from immortalised cell lines that lack the genetic diversity and histopathological heterogeneity of patient tumours. Spheroids generally fail to reproduce the original architecture of the ECM, vascular systems, and immune microenvironments. Their relatively simple organization limits their ability to model complex tumor evolution, immune escape, and organ-specific metastasis. Therefore, while spheroids are highly suitable for preliminary mechanistic studies and high-throughput screening, their predictive value for clinical responses remains limited [5].
Compared with spheroids, tumor organoids exhibit substantially higher physiological relevance and patient specificity. Organoids are commonly derived from patient tumor tissues, cancer stem cells, or pluripotent stem cells and can preserve important histological, genomic, and phenotypic characteristics of primary tumors. Therefore, organoids are suitable for studying inter-tumour heterogeneity and predicting individual responses to therapy. PDOs have shown good results in precision oncology to date and are being applied to drug sensitivity testing, companion diagnostics, and the construction of organoid biobanks. Organoids can replicate the structure, differentiation status, and lineage hierarchy of glandular tissue in original cultures more accurately than traditional spheroids [50].
Organoid systems still have the following problems, however. First, the establishment efficiency of organoids differs among different types of tumors, and some tumors are not conducive to long-term culture. Second, most organoid cultures are based on animal-derived matrices such as Matrigel, and they have batch-to-batch variability and limited biochemical control. Third, extended passage may result in clonal selection and genetic drift, thus changing the original tumour heterogeneity over time [51,52]. Conventional organoid systems are often deficient in vascular, neural, and immune components and are thus unable to accurately mimic the systemic tumor-host interaction and immunotherapy response [53].
Tumour-on-a-chip systems are currently one of the most advanced types of 3D biomimetic tumour models. Microfluidics and tissue engineering/living cell culture have been combined to create dynamic platforms that can simulate many necessary conditions of the TME, such as continuous perfusion, shear stress, endothelial barriers, immune cell migration, and spatiotemporal signaling gradients. Tumour-on-a-chip devices can simulate the progression of tumours, angiogenesis, and metastasis more realistically compared with static culture systems, as well as drug transport. Multi-organ-on-a-chip systems can also be used to study organ-specific metastasis and systemic drug toxicity in a novel way [54].
Although they have the above advantages, tumor-on-a-chip technologies still have some practical problems. Microfluidic platform construction and use require advanced engineering knowledge and specialized facilities; thus, they are relatively difficult to obtain and scale up. Chip design complexity may also reduce throughput and reproducibility. Many cells are present in different amounts and in different environments within the same well. Although tumour-on-a-chip devices are highly biomimetic, they are still relatively expensive to produce on a large scale and have not been widely used in clinical practice due to a lack of standardised manufacturing [55].
The three general 3D biomimetic tumor models have their own strengths and weaknesses and thus are suitable for different research purposes. Tumor spheroids are suitable for rapid and cost-effective drug screening, tumor organoids can maintain the patient-specific heterogeneity of tumors and support precision medicine, and tumor-on-a-chip systems are particularly good at reconstructing dynamic physiological microenvironments and multicellular interactions. Instead of being competing technologies, the models should be considered as supplementary means that together improve the accuracy and applicability of preclinical cancer research. Future improvements in biomaterials, vascular engineering, immune reconstruction and artificial intelligence will be integrated with the strengths of the above systems to promote the development of next-generation tumour model platforms [56, 57].
Applications of in vitro reconstructed 3D biomimetic tumor microenvironment models in tumor research
Compared with the former two-dimensional system, the new three-dimensional tumor model can partially reconstruct the environment of hypoxia, nutrient diffusion gradients, ECM remodeling, biomechanical signals and multicellular heterogeneity to provide more physiologically realistic platforms for studying cancer biology and drug responses. The three-dimensional systems for cancer research are also different in strength. Tumor spheroids are generally simple and reproducible, so they have been widely employed for drug screening and studies of cancer stem cells. Tumour organoids can maintain the patient’s original histology and molecular characteristics better, so they are now frequently employed in precision oncology and therapeutic prediction. Now, microfluidic perfusion and vascular interfaces have been added to the tumour-on-a-chip platform to construct dynamic models of tumour growth and metastasis, as well as drug delivery [58,59].
The following sections introduce some representative applications of 3D biomimetic tumour models in drug screening, tumour heterogeneity research, metastasis, therapeutic resistance and immunotherapy evaluation.
Drug screening and precision medicine
3D biomimetic tumour models have been applied widely in the screening of anticancer drugs and precision oncology due to their excellent representation of the architecture, cellular heterogeneity, and therapeutic response of tumours in vivo. High-end 3D systems have provided new platforms for the investigation of drug sensitivity and resistance in all types of cancer, and also advanced individualised treatment strategies; they are no longer limited to traditional 2D cultures [60].
Tumour spheroids have recently been employed in high-throughput drug screening due to their ability to replicate diffusion gradients and multicellular drug resistance in solid tumours to some extent. Faezeh Ghasemi, et al. [61] Established colorectal cancer spheroids using HCT116 and SW620 cells, and showed that a combined treatment of aspirin and LGK974 inhibited tumour invasion and promoted apoptosis by suppressing the Wnt and MAPK signalling pathways. Based on the above results, it can be seen that 3D spheroid systems are suitable for recreating microenvironments and studying how signaling-related drug resistance occurs mechanistically.
Compared with spheroid systems, PDOs have shown more physiological relevance and thus stronger predictive power for personalised medicine. Fuchou Tang, et al. [62] Established colorectal cancer organoids that have maintained the morphological and molecular heterogeneity of primary tumours. In combination with computational drug prediction and high-throughput screening of many compounds, organoids have also uncovered many new drug candidates for colorectal cancer. Importantly, the drug response profiles of the organoids were in line with those in paired patient-derived xenograft models; thus, PDOs platforms may be suitable tools for personalised treatment prediction and translational oncology research.
Tumor-on-a-chip systems can also be used to introduce dynamic perfusion, variable biochemical gradients and microfluidic drug delivery for improved drug tests. Ji Lin, et al. [4]. Developed a microfluidic chip with herringbone structures and a three-dimensional micropillar array to quickly form uniformly sized colon cancer spheroids. Concentration-gradient generators were incorporated into the chip platform to perform dynamic and high-throughput drug sensitivity analysis, and interpatient differences in therapeutic response were successfully identified. Therefore, it has been determined that the platform for tumor-on-a-chip could accurately screen drugs and assess patients.
Recently, some researchers have also been conducting organoid-based drug screening for other types of tumours. Patient-derived organoids for breast cancer have shown excellent predictive ability for chemotherapy sensitivity and therapeutic response [63]. Organoid-based drug sensitivity tests for lung cancer have also been used to predict the response of advanced lung cancer patients to chemotherapy and targeted therapy [64]. Organoid biobanks of gastric cancer research have been established to preserve histological and genetic heterogeneity for large-scale therapeutic screening and personalised treatment studies [65].
Tumor heterogeneity and cancer stem cell research
First of all, tumours are not the same, and therefore a single drug cannot treat all of them. Based on the above, multiple studies have shown that both intertumoral heterogeneity (variations among tumors from different patients) and intratumoral heterogeneity (different genetic and phenotypic subpopulations within a single tumor) are involved in the progression, spread, immune evasion and drug resistance of cancer [66]. Traditional 2D culture systems are unable to maintain the complexity of these tumours, and prolonged monolayer culture often leads to clonal selection, phenotypic uniformity and the loss of the original tumour structure. At the same time, three-dimensional biomimetic tumor models are also available to provide more representative microenvironments for in vitro experiments and can maintain some of the cellular heterogeneity, spatial organisation and dynamic cell-to-cell interactions of live tumours.
Among the current 3D systems, tumor organoids have shown good results in preserving the heterogeneity of patient-specific tumours. PDOs can retain some histopathological features, genomic mutations, transcriptional profiles and differentiation hierarchies of primary tumours for a relatively short time in culture. Some research has successfully built organoid biobanks to study interpatient heterogeneity across multiple malignancies, including colorectal, breast, prostate, gastric and ovarian cancers. Additionally, PDOs derived from different patients often exhibit distinct drug sensitivities, enabling more precise drug selection for personalised cancer treatment. Organoid-based platforms can also be used to study the development and drug response of tumours over an extended period [31].
Tumor spheroids have also been used extensively to study the heterogeneity of tumours and CSCs. CSCs are a small subset of tumour cells that possess self-renewal, differentiation, and tumour-initiating abilities, and are considered a main cause of relapse, spread and treatment failure. Compared with 2D monolayer culture, tumorsphere culture in a non-adherent environment preferentially enriches stem-like cancer cell populations and promotes the expression of stemness-associated markers such as CD44, CD133, SOX2, NANOG and OCT4. Importantly, the hypoxic and nutrient-deprived microenvironment that forms in spheroids is similar to the niche for CSCs in vivo; therefore, studies on stemness maintenance and therapy resistance mechanisms have been carried out [67].
New evidence has shown that three-dimensional tumour models are now used to investigate cellular plasticity and other dynamic phenotypic changes in tumours during their development. In recent years, EMT and mesenchymal-epithelial transition (MET) have also been recognized as highly plastic and reversible phenomena that are regulated by microenvironmental cues rather than fixed cell states. By strengthening the stiffness of the extracellular matrix, rearranging the three-dimensional distribution of oxygen and altering stromal-cell interactions, and so on, novel approaches have been proposed to investigate the effects of biomechanical and metabolic signals on the plasticity, invasiveness and metastasis of cancer cells. Multicellular 3D models of fibroblasts, endothelial cells and immune cells can also be used to study paracrine signalling networks involved in the differential response to therapy[68].
In recent years, with the development of single-cell sequencing and spatial transcriptomics, 3D tumour models have also been applied more frequently in research on heterogeneity. The above technologies can perform high-resolution characterisation of clonal evolution, lineage trajectories and cell-state transitions in reconstructed tumour ecosystems. In conjunction with patient-derived organoids and tumor-on-a-chip platforms, multiomics will be used to study the progression of tumors and advance the development of personalised treatments [69].
Tumor metastasis and therapeutic resistance
Metastasis and therapeutic resistance in cancer treatment remain serious issues; these problems are often associated with tumour heterogeneity, remodelling of the extracellular matrix, metabolic adaptation, dynamic tumour-microenvironment interaction, etc [70]. Conventional 2D culture systems are unable to replicate the above complex biological processes, and 3D biomimetic tumor models provide more physiologically relevant platforms for studying metastatic dissemination, drug penetration, EMT and therapy resistance mechanisms.
Tumor spheroids have been used to study the role of microenvironmental stress and metabolic reprogramming in the progression of cancer invasion and metastasis. Hyonchol Jang, et al. [71] cultured breast cancer cells under spheroid and re-adherent conditions to simulate circulating tumor cells and metastatic tumor formation. Their study demonstrated that cholesterol biosynthesis pathways were significantly upregulated during spheroid formation and metastatic transition, and inhibition of cholesterol synthesis markedly reduced invasive capacity. Therefore, these studies have shown that 3D spheroid systems can be used to study the metabolic changes of metastasis and find new anti-metastatic drugs.
Patient-derived organoids have also demonstrated the ability to study therapeutic resistance and personalised treatment responses. Chuxia Deng et al. [63]. Used breast cancer organoids as real-time platforms for the study of personalised therapeutic strategies in refractory breast cancer. The patterns of drug sensitivity in the organoids closely matched those of patients previously treated with drugs, and some clinical cases successfully predicted the effect of treatment. The above results provide further support for applying organoid systems in precision oncology and resistance-associated therapeutic stratification.
Tumor-on-a-chip platforms have certain advantages over static culture systems in studying dynamic metastatic processes and vascular invasion. Chwee Teck Lim, et al. [72] Combined a tumour trans-endothelial migration chip with machine learning algorithms to study exosome-mediated endothelial invasion in breast cancer. High-throughput microfluidic analysis was carried out in this study, and it was found that exosomes secreted by highly metastatic breast cancer cells can disrupt endothelial junctions and induce EMT to promote the spread and dissemination of tumours. Importantly, the integration of machine learning and microfluidic tumor platforms has achieved high-accuracy prediction of invasion potential based on biomarker combinations, and thus, artificial intelligence-assisted tumor models for metastasis research are emerging.
Many other kinds of cancer have been studied, and all of them have shown that three-dimensional biomimetic systems are effective in investigating drug resistance. Tumor spheroid models have been widely used in glioblastoma to study cancer stem cell-associated radioresistance and recurrence mechanisms [73]. Prostate cancer single-cell organoids have shown the heterogeneity of tumours and enabled personalised treatment studies to date [74]. Organoid-based drug sensitivity tests for lung cancer have also shown good predictive ability of clinical response to chemotherapy and targeted therapy [64]. Biorepository for organoid biobanks of gastric cancer that preserve regional heterogeneity and subclonal architecture have enabled mechanistic studies of tumour evolution and therapeutic resistance [65].
In short, all of the above studies have shown that 3D biomimetic tumour models are more physiologically relevant platforms for research on tumour progression, metastatic dissemination, therapeutic resistance and personalised drug responses. By partially reconstructing the structural, biochemical and mechanical characteristics of the native tumour microenvironment in 3D systems, many new paths for the mechanistic study of cancer have been opened, and the development of precision medicine in oncology has also advanced rapidly.
Immune microenvironment modeling and immunotherapy evaluation
The immune microenvironment in tumours promotes the development of tumours, spread of metastasis and resistance to therapy. More and more studies have shown that interaction among tumor cells, immune cells, stroma and extracellular matrix components all work together to promote immune evasion and therapy resistance. Therefore, one of the purposes of creating an artificial immune-related tumour microenvironment in a three-dimensional biomimetic tumour model has been to build an advanced one [11].
Compared with the old way of 2D culture, a new 3D tumour model can be used to study how the immune system works in tumours. Traditional monolayer cultures lack spatial organisation, an extracellular matrix and cytokine gradients, so they are not conducive to studying immune cell infiltration and activation. Multicellular tumor spheroids and organoids, on the other hand, can partially reproduce the structure and biochemistry of actual tumors to study immune suppression, macrophage polarisation and T-cell dysfunction in a hypoxic tumour microenvironment [75].
Recently, in the field of immune co-culture systems for tumor organoids and tumor-infiltrating lymphocytes (TILs), peripheral blood lymphocytes, and macrophages, researchers have been conducting immunotherapeutic response studies. The above systems have shown good results in studies of immune checkpoint blockade and personalised immunotherapy [76, 77]. Tumor-on-a-chip platforms have also improved the model of the immune system by introducing microfluidic perfusion, vascular barriers and dynamic immune cell trafficking to achieve real-time observation of immune cell migration and tumour infiltration [78].
3D immune-related tumour models have also provided new ways to investigate the reasons for immunotherapy resistance. Hypoxia, extracellular matrix stiffness and immunosuppressive stromal signals can all reduce the strength of the T-cell response to treatment. Based on the above reconstruction of microenvironmental conditions, advanced 3D systems can be employed to study tumor immune escape and identify predictive biomarkers for immunotherapy.
3D bioprinting and vascularized tumor models
Although current 3D tumour models have improved in reconstruction of the tumour microenvironment, lack of vascularisation and poor spatial organisation are still prominent problems. Recently, 3D bioprinting technology has begun to be used to build high-regulation and biomimetic tumour structures. Precise placement of tumor cells, stromal cells, ECM components and bioactive materials in specific regions is achieved by 3D bioprinting, and a complex multicellular tumor ecosystem with good structural accuracy can be constructed.
Importantly, vascularized tumor models generated through bioprinting and microengineering approaches can partially reproduce nutrient transport, oxygen gradients, and drug diffusion processes observed in vivo. The incorporation of perfusable vascular networks further improves the physiological relevance of tumor models and facilitates investigation of tumor angiogenesis, metastatic dissemination, and nanomedicine delivery. In addition, bioprinted tumor systems provide highly customizable platforms for patient-specific disease modeling and therapeutic evaluation [79,80].
Multiomics-integrated tumor modeling
Recently, many omics technologies have strengthened the analysis power of three-dimensional biomimetic tumour models. Single-cell RNA sequencing (scRNA-seq), spatial transcriptomics, proteomics, metabolomics and epigenomic profiling can now be used to investigate the high-resolution features of the tumor ecosystem at the cellular and molecular levels [81]. All three ways above are more extensive than traditional bulk analysis in providing data on clonal evolution, cellular plasticity, metabolic adaptation and the tumour microenvironment.
Recently, together with the construction of multi-omics data, patient-derived organoids and tumor-on-a-chip systems have also been used to study tumour heterogeneity and drug resistance [82]. Spatial transcriptomics can also be applied to study changes in gene expression in different areas of intact tumours to uncover the spatial organisation of signalling pathways and cell-state transitions. Lineage tracing and organoid platforms can be used to study how tumours change after treatment dynamically.
Artificial intelligence-assisted tumor modeling
Artificial intelligence (AI) and machine learning technology are being applied increasingly widely to all aspects of three-dimensional tumour research in recent years, such as data analysis and drug discovery in precision oncology. In conjunction with AI algorithms, organoid biobanks, tumor-on-a-chip systems and high-content imaging platforms are now used to identify differences in response and drug sensitivity among various types of tumours more efficiently.
Many problems in the research of disease phenotype and biomarkers have been addressed by machine learning. Employ AI-aided computational models for virtual experiments to accelerate the speed of drug discovery and reduce the number of experiments by simulating tumour growth and drug response. AI can also be used to analyze various ‘-omics’ data to improve the prediction accuracy of personalised medicine and advance the development of personalised medicine [56].
Current challenges and clinical translation
Although 3D biomimetic models of tumours have progressed to some extent, many serious problems still need to be solved before they can be used broadly in clinical practice. First, the current 3D systems are still unable to fully reconstruct the complexity of the native tumor ecosystem, such as vascularisation, systemic immunity, neural regulation and long-term changes in the tumour [83]. Most in vitro models do not show the same changes in the dynamic interactions among cancer cells, the stroma, immune cells, microbiota, etc [84].
Second, the experiment is not uniform or reproducible. Changes in the materials of the extracellular matrix, culture environments, cell origin and production methods may lead to variations in model performance and treatment effects. Matrigel and other animal-derived matrices commonly used in organoid systems have batch-to-batch variations and are difficult to modify biochemically. In addition, tumor-on-a-chip platforms generally have complex fabrication procedures and specialized equipment, so they are not conducive to large-scale applications and interlaboratory reproducibility [84].
Third, the high cost and technical difficulty of advanced 3D systems continue to restrict their clinical application [85]. The construction of patient-derived organoids and integrated microphysiological systems generally requires high-level technical skills, prolonged culture periods and special analysis platforms. The norms for regulatory assessment of clinical translation are also not fully formed.
Despite these limitations, with the increasing application of vascular engineering, immune system reconstruction, bioprinting technology, multi-omics analysis and artificial intelligence in recent years, the biological authenticity and prognostic value of next-generation three-dimensional tumour models are expected to be substantially improved. With the continuous development of technology and standards, the next generation of 3D biomimetic tumour systems will be good platforms for mechanistic research on cancer, drug discovery and personalised medicine.
As shown in the previous descriptive report, only an individual 3D tumour model was described; this time, however, three typical biomimetic tumour systems are systematically compared based on their ability to reconstruct the TME, show the different functions of these systems at various stages of cancer research, and put forward an interdisciplinary strategy to address problems in clinical translation. Partial reconstruction of tumor architecture, extracellular matrix interactions, biochemical gradients and multicellular communication are also utilized in the above models to conduct in-depth studies on tumor development, spread, treatment resistance and immune evasion. Tumor spheroids, organoids and tumor-on-a-chip systems are all more representative of various aspects of tumour biology compared with traditional monolayer cultures; together they offer complementary tools for mechanistic studies and translational oncology research.
Tumor spheroids are relatively simple and inexpensive, so they have been applied widely to drug screening and studies of cancer stem cells in 3D systems recently. Tumour organoids are better at preserving patient-specific histopathological and molecular characteristics, and thus show promise for precision medicine and personalised therapeutic prediction. Tumor-on-a-chip platforms have added microfluidic perfusion, vascular interfaces and dynamic mechanical stimulation to construct an artificial tumour microenvironment more closely mimicking that in vivo for real-time monitoring of tumour-microenvironment interactions.
Recently, with the development of bioprinting technology, multi-omics analysis and artificial intelligence, etc., many functions have been added to 3D tumour models. The combination of the above new technologies is accelerating the construction of more physiologically realistic, immune-competent and patient-specific tumour systems [85]. However, the following problems have not been solved: lack of standardisation, incomplete reconstruction of the systemic tumour ecosystem, high technical complexity, and limited clinical scalability.
Overall, 3D biomimetic tumor models are gradually evolving from simplified experimental tools into comprehensive platforms for mechanistic cancer research, drug development, and precision oncology. With continued interdisciplinary advances in biomaterials, bioengineering, computational biology, and translational medicine, next-generation 3D tumor models are expected to further improve the prediction of therapeutic responses and facilitate the clinical implementation of personalized cancer treatment strategies.
CRediT authorship contribution statement
Yinuo Ma: Writing – review & editing, Writing – original draft, Visualization, Project administration, Conceptualization. Yili Sun: Supervision. Jia Li: Funding acquisition.
Declaration of competing interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
This work was supported by grants from National Natural Science Foundation of China (82570641, 82504593), Natural Science Foundation of Shanghai (24ZR1477400), Taishan Scholar Foundation of Shandong Province (tstp0648, China), Shandong Provincial Natural Science Foundation (ZR2024QC286). Key R&D Program of Shandong Province, China (2024CXPT028, 2024CXGC010619). Innovative Drug Research and Development National Science and Technology Major Project (2025ZD1800700).
Data availability: Data will be made available on request.
- Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74(3):229-63. Available from: https://doi.org/10.3322/caac.21834
- Mazzocchi A, Soker S, Skardal A. 3D bioprinting for high-throughput screening: drug screening, disease modeling, and precision medicine applications. Appl Phys Rev. 2019;6(1). Available from: https://doi.org/10.1063/1.5056188
- Yang Q, Li M, Yang X, et al. Flourishing tumor organoids: history, emerging technology, and application. Bioeng Transl Med. 2023;8(5):e10559.Available from: https://doi.org/10.1002/btm2.10559
- Zhou G, Lin X, Li H, et al. Assessment of drug treatment response using primary human colon cancer cell spheroids cultivated in a microfluidic mixer chip. Biosens Bioelectron. 2025;269:116944. Available from: https://doi.org/10.1016/j.bios.2024.116944
- Cordeiro S, Oliveira BB, Valente R, et al. Breaking the mold: 3D cell cultures reshaping the future of cancer research. Front Cell Dev Biol. 2024;12:1507388. Available from: https://doi.org/10.3389/fcell.2024.1507388
- Esposito A, Ferraresi A, Vallino L, et al. Three-dimensional in vitro cell cultures as a feasible and promising alternative to two-dimensional and animal models in cancer research. Int J Biol Sci. 2024;20(13):5293-311. Available from: https://doi.org/10.7150/ijbs.96469
- Fridman WH, Zitvogel L, Sautés-Fridman C, et al. The immune contexture in cancer prognosis and treatment. Nat Rev Clin Oncol. 2017;14(12):717-34.
- Sahai E, Astsaturov I, Cukierman E, et al. A framework for advancing our understanding of cancer-associated fibroblasts. Nat Rev Cancer. 2020;20(3):174-86. Available from: https://doi.org/10.1038/s41568-019-0238-1
- Schreiber RD, Old LJ, Smyth MJ. Cancer immunoediting: integrating immunity's roles in cancer suppression and promotion. Science. 2011;331(6024):1565-70. Available from: https://doi.org/10.1126/science.1203486
- Bruni D, Angell HK, Galon J. The immune contexture and Immunoscore in cancer prognosis and therapeutic efficacy. Nat Rev Cancer. 2020;20(11):662-80. Available from: https://doi.org/10.1038/s41568-020-0285-7
- Li W, Zhou Z, Zhou X, et al. 3D biomimetic models to reconstitute tumor microenvironment in vitro: spheroids, organoids, and tumor-on-a-chip. Adv Healthc Mater. 2023;12(18):e2202609. Available from: https://doi.org/10.1002/adhm.202202609
- Sutherland RM, McCredie JA, Inch WR. Growth of multicell spheroids in tissue culture as a model of nodular carcinomas. J Natl Cancer Inst. 1971;46(1):113-20.
- Costa EC, Gaspar VM, Coutinho P, et al. Optimization of liquid overlay technique to formulate heterogenic 3D co-cultures models. Biotechnol Bioeng. 2014;111(8):1672-85. Available from: https://doi.org/10.1002/bit.25210
- Costa EC, Moreira AF, de Melo-Diogo D, et al. 3D tumor spheroids: an overview on the tools and techniques used for their analysis. Biotechnol Adv. 2016;34(8):1427-41. Available from: https://doi.org/10.1016/j.biotechadv.2016.11.002
- Han SJ, Kwon S, Kim KS. Challenges of applying multicellular tumor spheroids in preclinical phase. Cancer Cell Int. 2021;21(1):152.Available from: https://doi.org/10.1186/s12935-021-01853-8
- Qu J, Kalyani FS, Liu L, et al. Tumor organoids: synergistic applications, current challenges, and future prospects in cancer therapy. Cancer Commun (Lond). 2021;41(12):1331-53. Available from: https://doi.org/10.1002/cac2.12224
- Friedrich J, Seidel C, Ebner R, et al. Spheroid-based drug screen: considerations and practical approach. Nat Protoc. 2009;4(3):309-24. Available from: https://doi.org/10.1038/nprot.2008.226
- Sato T, Vries RG, Snippert HJ, et al. Single Lgr5 stem cells build crypt-villus structures in vitro without a mesenchymal niche. Nature. 2009;459(7244):262-5. Available from: https://doi.org/10.1038/nature07935
- Sato T, Stange DE, Ferrante M, et al. Long-term expansion of epithelial organoids from human colon, adenoma, adenocarcinoma, and Barrett's epithelium. Gastroenterology. 2011;141(5):1762-79. Available from: https://doi.org/10.1053/j.gastro.2011.07.050
- Qu S, Xu R, Yi G, et al. Patient-derived organoids in human cancer: a platform for fundamental research and precision medicine. Mol Biomed. 2024;5(1):6. Available from: https://doi.org/10.1186/s43556-023-00165-9
- Chew CA, Wun CM, Lee YF, et al. Functional precision in pancreatic cancer: redefining biomarkers with patient-derived organoids. Int J Mol Sci. 2025;26(18). Available from: https://doi.org/10.3390/ijms26189083
- Sachs N, de Ligt J, Kopper O, et al. A living biobank of breast cancer organoids captures disease heterogeneity. Cell. 2018;172(1-2):373-86.e10. Available from: https://doi.org/10.1016/j.cell.2017.11.010
- Kim M, Mun H, Sung CO, et al. Patient-derived lung cancer organoids as in vitro cancer models for therapeutic screening. Nat Commun. 2019;10(1):3991. Available from: https://doi.org/10.1038/s41467-019-11867-6
- Mullenders J, de Jongh E, Brousali A, et al. Mouse and human urothelial cancer organoids: a tool for bladder cancer research. Proc Natl Acad Sci U S A. 2019;116(10):4567-74. Available from: https://doi.org/10.1073/pnas.1803595116
- Kopper O, de Witte CJ, Lõhmussaar K, et al. An organoid platform for ovarian cancer captures intra- and interpatient heterogeneity. Nat Med. 2019;25(5):838-49. Available from: https://doi.org/10.1038/s41591-019-0422-6
- Shi R, Radulovich N, Ng C, et al. Organoid cultures as preclinical models of non-small cell lung cancer. Clin Cancer Res. 2020;26(5):1162-74. Available from: https://doi.org/10.1158/1078-0432.ccr-19-1376
- Wensink E, Bond M, Kucukkose E, et al. A review of the sensitivity of metastatic colorectal cancer patients with deficient mismatch repair to standard-of-care chemotherapy and monoclonal antibodies, with recommendations for future research. Cancer Treat Rev. 2021;95:102174. Available from: https://doi.org/10.1016/j.ctrv.2021.102174
- Xu H, Jiao Y, Qin S, et al. Organoid technology in disease modelling, drug development, personalized treatment and regeneration medicine. Exp Hematol Oncol. 2018;7:30. Available from: https://doi.org/10.1186/s40164-018-0122-9
- Di Paola FJ, Calafato G, Piccaluga PP, et al. Patient-derived organoid biobanks for translational research and precision medicine: challenges and future perspectives. J Pers Med. 2025;15(8). Available from: https://doi.org/10.3390/jpm15080394
- Xu J, Feng Q, Xia Y, et al. Organoids glimpse: the nexus for diverse tumor heterogeneity. Front Cell Dev Biol. 2026;14:1817560. Available from: https://doi.org/10.3389/fcell.2026.1817560
- Bai M, Liu M, Wang S, et al. Organoids in cancer therapy: translational applications and clinical promise. Mol Cancer. 2026.
- Huh D, Matthews BD, Mammoto A, et al. Reconstituting organ-level lung functions on a chip. Science. 2010;328(5986):1662-8. Available from: https://doi.org/10.1126/science.1188302
- Bhise NS, Manoharan V, Massa S, et al. A liver-on-a-chip platform with bioprinted hepatic spheroids. Biofabrication. 2016;8(1):014101. Available from: https://doi.org/10.1088/1758-5090/8/1/014101
- Zhang YS, Arneri A, Bersini S, et al. Bioprinting 3D microfibrous scaffolds for engineering endothelialized myocardium and heart-on-a-chip. Biomaterials. 2016;110:45-59. Available from: https://doi.org/10.1016/j.biomaterials.2016.09.003
- Ma LD, Wang YT, Wang JR, et al. Design and fabrication of a liver-on-a-chip platform for convenient, highly efficient, and safe in situ perfusion culture of 3D hepatic spheroids. Lab Chip. 2018;18(17):2547-62. Available from: https://doi.org/10.1039/c8lc00333e
- Ashammakhi N, Wesseling-Perry K, Hasan A, et al. Kidney-on-a-chip: untapped opportunities. Kidney Int. 2018;94(6):1073-86. Available from: https://doi.org/10.1016/j.kint.2018.06.034
- Kamei KI, Yoshioka M, Terada S, et al. Three-dimensional cultured liver-on-a-chip with mature hepatocyte-like cells derived from human pluripotent stem cells. Biomed Microdevices. 2019;21(3):73. Available from: https://doi.org/10.1007/s10544-019-0423-8
- Herland A, Maoz BM, Das D, et al. Quantitative prediction of human pharmacokinetic responses to drugs via fluidically coupled vascularized organ chips. Nat Biomed Eng. 2020;4(4):421-36. Available from: https://doi.org/10.1038/s41551-019-0498-9
- Jeon MS, Choi YY, Mo SJ, et al. Contributions of the microbiome to intestinal inflammation in a gut-on-a-chip. Nano Converg. 2022;9(1):8. Available from: https://doi.org/10.1186/s40580-022-00299-6
- Kohl Y, Biehl M, Spring S, et al. Microfluidic in vitro platform for (nano)safety and (nano)drug efficiency screening. Small. 2021;17(15):e2006012. Available from: https://doi.org/10.1002/smll.202006012
- Lee J, Mehrotra S, Zare-Eelanjekh E, et al. A heart-breast cancer-on-a-chip platform for disease modeling and monitoring of cardiotoxicity induced by cancer chemotherapy. Small. 2021;17(15):e2004258. Available from: https://doi.org/10.1002/smll.202004258
- Baek S, Yu SE, Deng YH, et al. Quenching epigenetic drug resistance using antihypoxic microparticles in glioblastoma patient-derived chips. Adv Healthc Mater. 2022;11(8):e2102226. Available from: https://doi.org/10.1002/adhm.202102226
- Lim J, Ching H, Yoon JK, et al. Microvascularized tumor organoids-on-chips: advancing preclinical drug screening with pathophysiological relevance. Nano Converg. 2021;8(1):12. Available from: https://doi.org/10.1186/s40580-021-00261-y
- Papamichail L, Koch LS, Veerman D, et al. Organoids-on-a-chip: microfluidic technology enables culture of organoids with enhanced tissue function and potential for disease modeling. Front Bioeng Biotechnol. 2025;13:1515340. Available from: https://doi.org/10.3389/fbioe.2025.1515340
- Azim MMN, Bhajan SK, Park JH, et al. Stem cell-derived organoids for cancer therapy: precision medicine and drug selection. Int J Mol Sci. 2026;27(7).
- Gaebler D, Hachey SJ, Hughes CCW. Improving tumor microenvironment assessment in chip systems through next-generation technology integration. Front Bioeng Biotechnol. 2024;12:1462293. Available from: https://doi.org/10.3389/fbioe.2024.1462293
- Liu L, Wang H, Chen R, et al. Cancer-on-a-chip for precision cancer medicine. Lab Chip. 2025;25(14):3314-47. Available from: https://doi.org/10.1039/d4lc01043d
- Kim H, Cho SW, Kim HN. Vascularized tumor-on-a-chip model as a platform for studying tumor-microenvironment-drug interaction. Macromol Biosci. 2025;25(10):e00240. Available from: https://doi.org/10.1002/mabi.202500240
- Lonkwic KM, Zajdel R, Kaczka K. Unlocking the potential of spheroids in personalized medicine: a systematic review of seeding methodologies. Int J Mol Sci. 2025;26(13). Available from: https://doi.org/10.3390/ijms26136478
- Tan X, Huang B, Yang X, et al. Construction and application of pancreatic exocrine organoid and spheroid for drug screening and precision medicine. Front Cell Dev Biol. 2025;13:1746622. Available from: https://doi.org/10.3389/fcell.2025.1746622
- Fatehullah A, Tan SH, Barker N. Organoids as an in vitro model of human development and disease. Nat Cell Biol. Available from: 2016;18(3):246-54. https://doi.org/10.1038/ncb3312
- Drost J, Clevers H. Organoids in cancer research. Nat Rev Cancer. 2018;18(7):407-18. Available from: https://doi.org/10.1038/s41568-018-0007-6
- Fan X, Hou K, Liu G, et al. Strategies to overcome the limitations of current organoid technology—engineered organoids. J Tissue Eng. 2025;16:20417314251319475. Available from: https://doi.org/10.1177/20417314251319475
- Lipreri MV, Totaro MT, Baldini N, et al. From spheroids to tumor-on-a-chip for cancer modeling and therapeutic testing. Micromachines. 2025;16(12). Available from: https://doi.org/10.3390/mi16121343
- Wang LX, Liu SL, Wu N. Application and development of organ-on-a-chip technology in cancer therapy. Front Oncol. 2025;15:1643230. https://doi.org/10.3389/fonc.2025.1643230
- Momoli C, Costa B, Lenti L, et al. The evolution of anticancer 3D in vitro models: the potential role of machine learning and AI in the next generation of animal-free experiments. Cancers. 2025;17(4). Available from: https://doi.org/10.3390/cancers17040700
- Chen J, Yang H. Convergent bioprinting and microfluidics: toward next-generation biomimetic tumor models. Hepatobiliary Surg Nutr. 2026;15(1):18. Available from: https://doi.org/10.21037/hbsn-2026-1-0021
- Manduca N, Maccafeo E, De Maria R, et al. 3D cancer models: one step closer to in vitro human studies. Front Immunol. 2023;14:1175503. Available from: https://doi.org/10.3389/fimmu.2023.1175503
- Sharma K, Dey S, Karmakar R, et al. A comprehensive review of 3D cancer models for drug screening and translational research. Cancer Innov. 2024;3(1):e102. Available from: https://doi.org/10.1002/cai2.102
- Guan X, Huang S. Advances in the application of 3D tumor models in precision oncology and drug screening. Front Bioeng Biotechnol. 2022;10:1021966. Available from: https://doi.org/10.3389/fbioe.2022.1021966
- Bagheri M, Tabatabae Far MA, Mirzaei H, et al. Evaluation of antitumor effects of aspirin and LGK974 drugs on cellular signaling pathways, cell cycle and apoptosis in colorectal cancer cell lines compared to oxaliplatin drug. Fundam Clin Pharmacol. 2020;34(1):51-64. Available from: https://doi.org/10.1111/fcp.12492
- Mao Y, Wang W, Yang J, et al. Drug repurposing screening and mechanism analysis based on human colorectal cancer organoids. Protein Cell. 2024;15(4):285-304. Available from: https://doi.org/10.1093/procel/pwad038
- Chen P, Zhang X, Ding R, et al. Patient-derived organoids can guide personalized therapies for patients with advanced breast cancer. Adv Sci. 2021;8(22):e2101176. Available from: https://doi.org/10.1002/advs.202101176
- Wang HM, Zhang CY, Peng KC, et al. Using patient-derived organoids to predict locally advanced or metastatic lung cancer tumor response: a real-world study. Cell Rep Med. 2023;4(2):100911. Available from: https://doi.org/10.1016/j.xcrm.2022.100911
- Yan HHN, Siu HC, Law S, et al. A comprehensive human gastric cancer organoid biobank captures tumor subtype heterogeneity and enables therapeutic screening. Cell Stem Cell. 2018;23(6):882-97.e11. Available from: https://doi.org/10.1016/j.stem.2018.09.016
- Zhang A, Miao K, Sun H, et al. Tumor heterogeneity reshapes the tumor microenvironment to influence drug resistance. Int J Biol Sci. 2022;18(7):3019-33. Available from: https://doi.org/10.7150/ijbs.72534
- Lamichhane A, Tavana H. Three-dimensional tumor models to study cancer stemness-mediated drug resistance. Cell Mol Bioeng. 2024;17(2):107-19. Available from: https://doi.org/10.1007/s12195-024-00798-y
- Coppo R, Inoue M. Patient-derived tumor organoids to model cancer cell plasticity and overcome therapeutic resistance. Cells. 2025;14(18). Available from: https://doi.org/10.3390/cells14181464
- Liu Y, Dai Y, Wang L. Spatial omics at the forefront: emerging technologies, analytical innovations, and clinical applications. Cancer Cell. 2026;44(1):24-49. Available from: https://doi.org/10.1016/j.ccell.2025.12.009
- Hanahan D. Hallmarks of cancer: new dimensions. Cancer Discov. 2022;12(1):31-46. Available from: https://doi.org/10.1158/2159-8290.cd-21-1059
- Kim HY, Bae SJ, Choi JW, et al. Cholesterol synthesis is important for breast cancer cell tumor sphere formation and invasion. Biomedicines. 2022;10(8). Available from: https://doi.org/10.3390/biomedicines10081908
- Zhang X, Bai JJ, Fan SC, et al. Dissecting exosomal-tumoral-vascular interactions of single tumor cells and clusters using a tumoral-transendothelial migration chip. ACS Nano. 2025;19(26):23680-92.
- Jo H, Lee S, Kim MH, et al. Recapitulating glioma stem cell niches using 3D spheroid models for glioblastoma research. Biosensors. 2024;14(11). Available from: https://doi.org/10.3390/bios14110539
- Pamarthy S, Sabaaawy HE. Patient-derived organoids in prostate cancer: improving therapeutic efficacy in precision medicine. Mol Cancer. 2021;20(1):125. Available from: https://doi.org/10.1186/s12943-021-01426-3
- Fitzgerald AA, Li E, Weiner LM. 3D culture systems for exploring cancer immunology. Cancers. 2020;13(1). Available from: https://doi.org/10.3390/cancers13010056
- Si Q, Tao S, Wu J, et al. Tumor organoids in immunotherapy: from disease modeling to translational research. J Immunother Cancer. 2025;13(7). Available from: https://doi.org/10.1136/jitc-2025-011733
- Wang Q, Yuan F, Zuo X, et al. Breakthroughs and challenges of organoid models for assessing cancer immunotherapy: a cutting-edge tool for advancing personalised treatments. Cell Death Discov. 2025;11(1):222. Available from: https://doi.org/10.1038/s41420-025-02505-w
- Chen X, Tan D, Liu S, et al. Applying microfluidic technology to interpret the tumor immune microenvironment and cancer immunotherapy. Cancer Biol Med. 2026;23(2):169-85. Available from: https://doi.org/10.20892/j.issn.2095-3941.2025.0541
- Poljak I, Chiappini C, Adriani G. Engineering perfusion to meet tumor biology: are vascularized tumor-on-a-chip models ready to drive therapy innovation? Lab Chip. 2026;26(5):1162-90.
- Menzani B, De Gea P, Gidrol X, et al. Vascularizing organoids-on-chip for perfused and personalized models. Lab Chip. 2026;26(6):1798-819. Available from: https://doi.org/10.1039/d5lc00890e
- Jose A, Kulkarni P, Thilakan J, et al. Integration of pan-omics technologies and three-dimensional in vitro tumor models: an approach toward drug discovery and precision medicine. Mol Cancer. 2024;23(1):50.Available from: https://doi.org/10.1186/s12943-023-01916-6
- Cao X, Xia C, Li C, et al. Organ-on-a-chip technology and global multi-omics: current applications and future directions. MedComm. 2026;7(2):e70603. Available from: https://doi.org/10.1002/mco2.70603
- Wolff L, Hendrix S. Rethinking Matrigel: the complex journey to matrix alternatives in organoid culture. Adv Sci. 2025;12(47):e08734. Available from: https://doi.org/10.1002/advs.202508734
- Du L, Yang H. Spatial omics in 3D culture model systems: decoding cellular positioning mechanisms and microenvironmental dynamics. J Transl Med. 2025;23(1):1356. Available from: https://doi.org/10.1186/s12967-025-07390-6
- Piotrowska U, Tsoi J, Singh P, et al. 3D bioprinting and artificial intelligence for tumor microenvironment modeling: a scoping review of models, methods, and integration pathways. Mol Pharm. 2025;22(10):5801-23. Available from: https://doi.org/10.1021/acs.molpharmaceut.5c01062